Measure and improve your grip strength
Those who have read Peter Attia’s book Outlive know that grip strength, along with VO2 max is one of the best indicators of how long you will live. You can measure your grip strength using a cheap dynamometer:

Here’s a chart of average grip strength for Americans, by age:
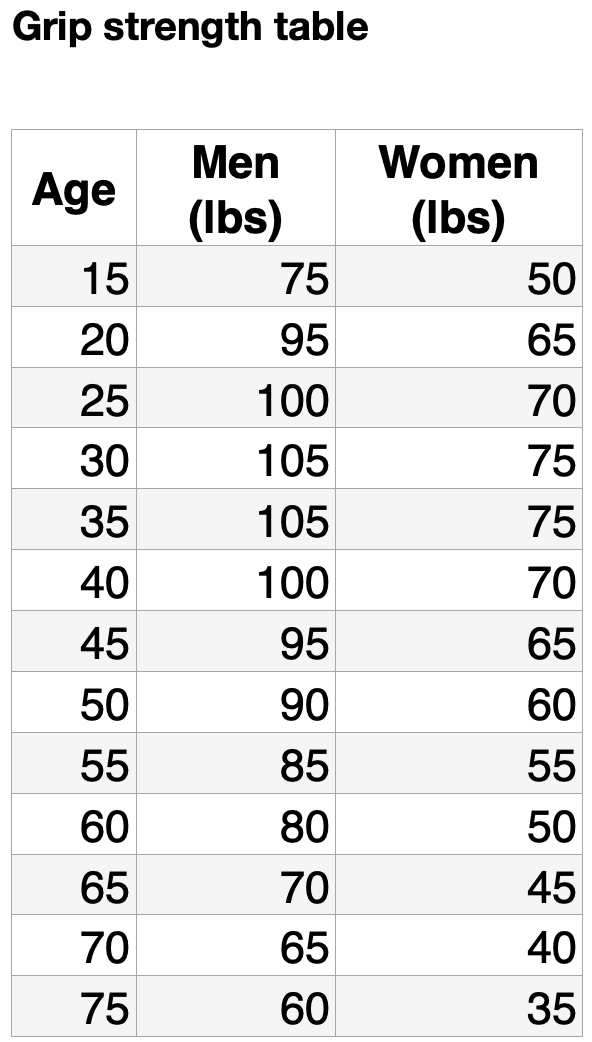
You want to improve grip strength. What you don’t want to do is get injured. Do NOT use something like this:

If you use this say five times a day, you’ll probably get tennis elbow, and that can hurt for months or even years. This is not the right tool for beginners. It should only be used twice a day max and is good for travel, not training at home.
Want to improve your grip strength? I have a program right here:
The Vital Role of Vaccines for Americans Over 60: Protecting Health and Independence

As we age, our immune systems naturally weaken, making adults over 60 more vulnerable to serious infections that can lead to hospitalization, disability, or even death. Vaccines are a cornerstone of preventive healthcare, offering robust protection against diseases that disproportionately affect older adults. For Americans over 60, staying up to date with recommended vaccines is critical to maintaining health, independence, and quality of life.
Below, I explain the key vaccines for this age group, their benefits, and their recommended priority based on current CDC guidelines, tailored to the U.S. context.
Shingles Vaccine (Shingrix): Very Strongly Recommended
Shingles, caused by the reactivation of the varicella-zoster virus, affects about 1 in 3 older adults, with risks increasing after age 50. The painful rash can lead to postherpetic neuralgia, a debilitating nerve pain condition that can last months or years. Shingrix, a two-dose vaccine for adults 50 and older, is over 90% effective at preventing shingles and its complications. In 2018, only 34.5% of Americans over 60 had received a shingles vaccine, underscoring the need for greater uptake. Given its high efficacy and the significant impact of shingles on quality of life, Shingrix is very strongly recommended for all adults over 60, even those who’ve had shingles or the older Zostavax vaccine. This vaccine has also shown promise in reducing dementia and possibly Alzheimer’s. Medicare and most insurance plans cover it, making access straightforward.
One word of warning: many people become briefly sick after the second dose. In my case, I slept for 40 hours straight and woke up just long enough to cancel all my appointments before going back to sleep. Don’t plan on doing anything after your second dose!
Pneumococcal Vaccine: Very Strongly Recommended
Pneumococcal disease, caused by Streptococcus pneumoniae, leads to pneumonia, meningitis, and bloodstream infections, which are particularly severe in older adults. About 1 in 20 pneumonia cases and 1 in 6 bacteremia cases in those over 65 are fatal. The CDC recommends a single dose of PCV20 or PCV21 for all adults 50 and older, with PCV15 followed by PPSV23 as an alternative for some. These vaccines reduce the risk of invasive pneumococcal disease by up to 85%, protecting against hospitalization and death. Given the high morbidity and mortality in this age group, pneumococcal vaccination is very strongly recommended. Medicare Part B covers these vaccines at no cost for those 65 and older, removing financial barriers.
Influenza (Flu) Vaccine: Strongly Recommended
The flu can be devastating for older adults, leading to complications like pneumonia and heart issues. Each year, flu causes thousands of hospitalizations and deaths among those over 65. High-dose or adjuvanted flu vaccines (e.g., Fluzone High-Dose, Fluad) are designed specifically for adults 65 and older, offering stronger protection than standard-dose vaccines. Annual vaccination reduces flu-related hospitalizations by about 40%. Due to the seasonal nature of flu and its severe impact, an annual flu shot is strongly recommended. Most insurance plans, including Medicare, cover it at no cost. While the flu shot isn’t perfect, it’s a small price to pay to help improve your odds against something bad happening.
COVID-19 Vaccine: Recommended
COVID-19 remains a significant threat, particularly for older adults, with those over 65 accounting for the majority of related deaths. Vaccination, including boosters, significantly reduces severe outcomes, though public skepticism persists. Those previously vaccinated against COVID-19 have greater protection than the unvaccinated, with studies showing up to 90% reduction in hospitalization risk for boosted individuals.
In my view, it’s an individual choice. I don’t think you need to get boosted every year, but it depends on your immune system, exposure, frailty, etc. If you live in a senior community, you should probably be more protected. I do think the vaccine helped a lot of older people become less sick, but I also think far too many people under 65 were vaccinated and many boosters may not be the solution. Discuss concerns with a healthcare provider to weigh benefits and risks.
RSV Vaccine: Recommended for Some
Respiratory syncytial virus (RSV) can cause severe respiratory illness in older adults, particularly those 75 and older or those 60–74 with risk factors like heart or lung disease. Vaccines like Arexvy, Abrysvo, or mRESVIA reduce severe RSV outcomes by about 80%. The CDC recommends RSV vaccination for all adults 75 and older and for those 60–74 with specific conditions. For others over 60, it’s optional based on shared clinical decision-making with a provider, given varying risk levels.
Tdap/Td Vaccine: Recommended for some
Tetanus and diphtheria are rare but serious, with tetanus causing painful muscle spasms and diphtheria leading to respiratory complications. Adults over 60 need a Td booster every 10 years, with a one-time Tdap dose (including pertussis protection) if not previously received, especially if around infants. These vaccines are highly effective, and tetanus prevention relies solely on vaccination. If you’re often out doing physical things in environments where you may get a puncture would, I would recommend it. If you’re in a senior community, I doubt it is worth the trouble. Td/Tdap coverage is typically available through Medicare Part D or insurance.
Summary
The situation with vaccines is similar to hormone therapy for women: Not enough people are getting the protection they need, mostly because they don’t think about it. For adults over 60, vaccines prevent debilitating illnesses that can erode independence, strain finances, and burden caregivers. They reduce healthcare costs by lowering hospitalization rates and protect communities by limiting disease spread. Most vaccines are covered by Medicare or insurance, and side effects are generally mild (e.g., soreness, fatigue). Consulting a healthcare provider ensures a tailored vaccination plan, accounting for health status and prior doses.
New here? Explore the blog, learn the facts, or get with the program.
Longevity lecture series
My name is David Siegel. I’m a longevity coach based in Washington, DC. I give 8 lectures on longevity:
Longevity overview (see below)
Hormone replacement for women (and men)
All about fat
Insulin sensitivity and diet
What we know about heart disease today
Supplements for longevity and fitness
Fitness and muscle building for strength and longevity
How to build bone and reverse osteoporosis in the gym
The first one, below, is free. I can give it live to your audience and take questions. After the first one, we have two options:
Short version
For $800, I can give three 90-minute lectures where I combine the topics like this:
Insulin sensitivity, fat, diet, and supplements
Heart disease and cardiofitness
Building muscle and bone in the gym
This is a lot to pack into 3 lectures. Most people will find it very challenging. I will have to cut the topics short and just try to answer people’s questions.
Long version
For $1400, I give the first lecture for free, and the next seven lectures are about 45 minutes plus Q&A. There’s time for discussion. A good schedule would be to do one per week.
Delivery
The best way to deliver these is in person. That means you need to pay my travel expenses. For most communities, this is too expensive, though some national senior-care companies are considering having me give one lecture per day every day for 8 days (4 days one week, 4 days the next).
A good way to do it is via Zoom. Get all your residents into your theater with a big screen and then have someone run Zoom and a mic on your end, and I present on the big screen and interact with people. That’s affordable and works well.
I can also pre-record everything and put the videos onto a platform a license them to you.
Watch the overview. If you’re interested in more lectures, use the form at the bottom of the page to get in touch.
The Obesity Epidemic: Fueled by the Standard American Diet

In the 1960s, America was lean: only about 13% of adults were obese, and roughly 45% were overweight or obese combined. Home-cooked meals and smaller portions were the norm. Many people smoked and few exercised. Dieting was common but obesity was not.
Then came the Standard American Diet — the SAD. High in sugars, refined carbs, and ultra-processed foods—the SAD is relentlessly improved each year to be tastier and cheaper. Any restaurant or store that wants Americans’ business must now compete at a very high level of satiety, deliciousness, and affordability.
The health picture has changed significantly. Now in 2025, 27 percent of U.S. adults are overweight, 39 percent are obese, and 9 percent are morbidly obese. And those numbers are rising — projections say 78 percent of Americans will be overweight or obese by 2030. The average American man, at 5’9”, has a BMI of 29 (200 lbs), while the average woman, at 5’4”, has a BMI of 28 (170 lbs).
Doctors aren’t immune — the 2007 Physicians Health Study reported that among 19,000 doctors, 40% were overweight (BMI 25–29.9) and 23% were obese (BMI ≥30).
This epidemic, costing $173 billion annually, is no longer just dietary or lifestyle-driven—it’s a spiral, with insulin resistance now the main driver. To understand the multiple causes, let’s look at the major factors driving obesity:
Insulin resistance
Dietary shifts
Price
Availability
Portion sizes
Sedentary lifestyles
Socioeconomic factors
Dietary belief systems that keep failing
Epigenetic factors
Let’s break these down.

Dietary shifts
In the 1960s, Americans ate home-cooked meals with whole foods—vegetables, lean meats, and minimal processing. In 2025, the SAD dominates, with 60% of calories from ultra-processed foods packed with added sugars (17% of daily intake, triple the recommended limit), and refined grains. Fast food and sugary drinks have replaced balanced meals, with lunch and dinner markets now dominated by fast-casual chains and drive-thrus offering high-calorie, low-satiety options. These foods, engineered for palatability and repeat business, drive overconsumption and fuel insulin resistance.
Insulin resistance
A minor factor in the 1960s, insulin resistance is now a central driver of the obesity epidemic. Diets high in refined sugars and carbohydrates cause repeated blood glucose spikes, desensitizing cells to insulin and promoting fat storage while increasing hunger. This spiral is worsened by pregnancy-related insulin resistance, which increases maternal weight gain and predisposes future children to obesity. The effect is nonlinear — once people get to a certain threshold, insulin resistance really kicks in and starts an ever-increasing spiral of weight gain and further progress toward diabetes, which has doubled since 1980. Insulin resistance, powered by highly processed foods, carbohydrate-rich products, and plenty of sugar in almost everything, is now the number one public health threat for Americans. It’s reversible simply by doing the opposite of what it took to get it — a low-carb diet, fewer calories, and plenty of exercise. Italians, who love their pastas and desserts, limit their portion sizes, get protein in every meal, and are far more physically active than Americans are.

Price
The cost of food has shifted dramatically since the 1960s, when whole foods were relatively affordable. Thanks to aggressive lobbying, agricultural subsidies for corn, soy, and sugar have made processed, calorie-dense foods like sugary snacks and fast food cheaper than fresh produce, whose prices have risen faster. A fast-food meal costs around $5, while a healthy meal with vegetables and protein can exceed $15. This price disparity pushes low-income households toward the SAD, exacerbating obesity rates and insulin resistance, as affordable foods are often the least satiating and most calorie-dense.
Availability
In the 1960s, grocery stores and home cooking were the norm. By 2025, food deserts — areas with limited access to fresh foods — plague low-income urban and rural communities, forcing reliance on convenience stores and fast-food outlets stocked with SAD staples. Fast-casual chains and vending machines are ubiquitous, offering quick, cheap, high-carb options. This lack of access to nutrient-dense foods, combined with the omnipresence of processed ones, drives overconsumption and perpetuates obesity, particularly in underserved populations. One consequence of highly available food is that people aren’t used to going hungry — a natural condition for 99 percent of human existence. People would be better off going hours at a time with a bit of hunger. While multi-day fasts tend to destroy muscle in proportion to fat, limiting windows for eating during the day can be very beneficial. Instead, we are surrounded by cheap, tasty food all day long.
Portion sizes
Portion sizes have ballooned since the 1960s, when a soda was 12 ounces and a burger 4 ounces. By 2025, fast-food meals routinely include 32-ounce drinks and 8–12-ounce burgers, often exceeding 1,000 calories. Restaurants and packaged foods have followed suit, with oversized servings marketed as value. All-you-can-eat restaurants are popular and encourage overeating. These larger portions, often low in satiety due to refined carbs, directly contribute to weight gain and insulin resistance.
Sedentary lifestyles
The 1960s featured active daily routines—manual jobs, walking, and chores. By 2025, Americans average 8+ hours of sitting daily, tied to desks, screens, and cars. Urban design discourages walking, and children prioritize gaming over outdoor play. This shift, entrenched since the 2000s, reduces movement and worsens insulin resistance, as inactive muscles become less responsive to insulin, promoting fat storage and amplifying the effects of calorie-dense diets.
Socioeconomic factors
In the 1960s, obesity was less stratified by income. Today, low-income adults face a 46 percent obesity rate compared to 34 percent for college graduates. Limited income, long work hours, and lower nutrition literacy drive reliance on cheap, calorie-dense SAD foods. Families don’t eat dinner together nearly as much as they did decades ago. Tasty deserts are common after both lunch and dinner.
Dietary belief systems and fads that keep failing
The 1980s–2000s low-fat craze, which vilified fats and promoted carb-heavy, low-satiety foods, misled consumers into overeating sugars and starches. Diet gurus like Dr Dean Ornish even used the president of the United States as a case study for a low-fat lifestyle, paving the way for more insulin resistance and weight gain. By 2025, despite the decline of low-fat dogma, new fads — extreme diets, detoxes, and processed “health” foods — persist, often backed by misleading marketing. These beliefs, rooted in oversimplified (or zero) science, fail to address satiety or insulin resistance, perpetuating poor dietary choices and obesity.

There’s no end to the number of bad — and popular — diet books on the market.
Epigenetic factors
Negligible in the 1960s, epigenetic changes are now a small but growing factor. By 2025, maternal obesity (over 25% of pregnant women) and insulin resistance alter fetal gene expression, increasing offspring’s obesity risk through mechanisms like DNA methylation. This generational effect, driven by the SAD and rising maternal health issues, compounds the epidemic, subtly amplifying vulnerability in a feedback loop with dietary and socioeconomic drivers.
Poor food choices at schools
The prevalence of poor dietary options in schools, often dominated by processed foods high in sugar, sodium, and unhealthy fats, has been a significant contributor to childhood obesity and related health issues. School lunches frequently include items like pizza and fries that are full of chemical additives. Nutrition experts like Dr. Mark Hyman and Dr. Marion Nestle have been vocal advocates for transforming school food systems to prioritize health. Hyman has pushed for initiatives like introducing salad bars, eliminating junk foods from menus, supporting farm-to-school programs, teaching cooking skills, and banning junk-food marketing targeting children. Nestle, a prominent nutritionist and food policy expert, has criticized the influence of the food industry on school meals, noting their high sodium and sugar content, and advocates for systemic changes such as stricter regulation of food additives and policies to promote healthier, less processed options. Their combined efforts emphasize the need for policy reforms and educational campaigns to foster healthier eating environments for students.
Summary
Americans are fatter than ever. Reversing this demands overhauling food systems, addressing inequities, and breaking the metabolic spiral. Mostly, it involves education and better availability of affordable, healthy foods. Don’t choose the default SAD, make better choices and transform yourself — become leaner, stronger, and help others get out of the dietary trap 70 percent of Americans find themselves in. This is a good video to continue your learning:
What's wrong with the senior-care market and what I plan to do about it:

I’ve been giving talks at senior communities around the DC area, meeting the administrators, residents, touring the facilities, giving talks. It’s disheartening. I can help most people over 50 live 5-20 years longer. But there isn’t much demand — yet.
In this essay, I’m going to make a number of observations, give some background, and suggest how we can help people over 50 live much higher-quality lives. At the end, I’ll explain how you can help turn this into a serious business, especially if you’re a marketer or investor.
Let’s start with what I think is going on …
People are aging very poorly. We are behaving ourselves to death. Life expectancy, already low in the US, is heading down. It's not about economics, it's that the healthcare system is designed to suck money out of people at the wrong time — after they have a catastrophic event — rather than prevent it. And it’s that Americans are consuming more delicious food and becoming less active. There are other factors involved, but the numbers are not pretty …

The US has by far the most expensive healthcare system in the world, spending $12,000 per person each year, and getting the worst results of the top 25 developed countries. People in China live longer than Americans for 10 percent of the price, not because their medical system is better but because Chinese people are used to hard work and stay active. Americans are spending more money to move less, and that’s what’s causing the problem.
Retirement communities are giving retirees what they want, not what they need. These communities are all very similar. They are very comfortable. The food is plentiful and delicious. They have “activities,” gentle yoga, a bit of movement. People lift 3-pound dumbbells or do some gentle water activities, pretending they are exercising. This is physical abuse — our bodies aren’t designed for it. Yet, if a retirement community advertised that they would get you down to a normal weight, work with you to build muscle, no sugar, no alcohol, get stronger, and no treats except on birthdays — no one would join that community. The company would either go out of business or they would have to convert back to what we have today, because people won’t buy future health, they want to buy comfort.
People over 60 are eating more and moving less. They aren't challenged. They are living peaceful, calm lives and eating cake. Citydwellers are in far more danger than if they would just go to a farm or a ranch and get a job as a helper.
Longevity nerds are very few and very visible. There is a very small number of longevity nerds, but they make a lot of noise. They are YouTube influencers, investors, conference-goers, entrepreneurs, and Facebook group starters. Even though Peter Attia’s book Outlive has been on the NYT bestseller list for two years now, the actual number of people interested in doing something to improve their health is remarkably small. There’s a real market here, but it’s just getting started.
Because of one very expensive and very bad study that made headlines in 2002, women don't know anything about hormone replacement. After 50, their estrogen and progesterone plummet, and many don't even talk with a doctor about trying to replace them. Most doctors are unqualified. So 95 percent of women aren't getting the many life-saving benefits of hormone therapy — a public health failure.
Seventy five percent of American adults are overweight or obese. They think it's normal to keep buying clothes in bigger sizes. When it comes time to start injecting insulin, they order their supplies and start doing it five times every day. I ask them: “Would you like to stop injecting?” They say, “Sure, of course.” Then I tell them it’s going to take hard work for 6-12 months and lose weight, and they say “Nah, I’ll pass.”
People don't know anything about insulin resistance. Insulin resistance increases your chances of heart disease, cancer, Alzheimer’s, and gaining weight. Most people are insulin resistant, unhealthy, and are taking idiotic dietary advice that makes them sicker. They think they got unlucky and got cancer, but they brought it on with a poor diet. Everyone over 60 should know his/her A1c number from a test in the last six months. When I ask how many know their A1c number, usually only one person raises a hand — the person who’s on medication for insulin resistance. Even the diabetics don’t know their A1c number, nor do the staff don’t know their own A1c numbers. This number should drive most of your health decisions.
No keto awareness. If more than 50 percent of residents are seriously overweight, then the facility needs a keto option and most of the residents should be on it. In my lectures, I ask people if they know what keto is and they all shake their heads, including the staff (many of whom should also be on a keto diet). They are getting the wrong advice.
If residents cared to get better, they could wear a button on their clothing at all times showing their A1c number. Not a badge of shame, but a badge of courage. As people get tested and their numbers change, they trade the button in for a new one, so people can see they are making progress. It also tells staff to remind them if they order carbs or sodas or desserts that they won’t be helping themselves get the next lower numbered button. Obviously, if people want to be diabetic, they won’t wear the button, but if you’re wearing the button, you’re asking the staff to help you make good choices.
Know your A1c number and show others you are working to lower it.
Half of all heart attacks and strokes occur before age 65, yet people in their 40s and 50s have no idea what's about to happen. They aren't taking care of themselves -- they are too busy. They think when they get a heart attack they were just unlucky, and that’s when they spend hundreds of thousands of dollars to try to go back the way they were before.
No bone-building programs. This is so easy to do, yet no one does it. To learn more, read my big essay on bone building and watch the accompanying video. I have many ideas how people can do this easily and cheaply.
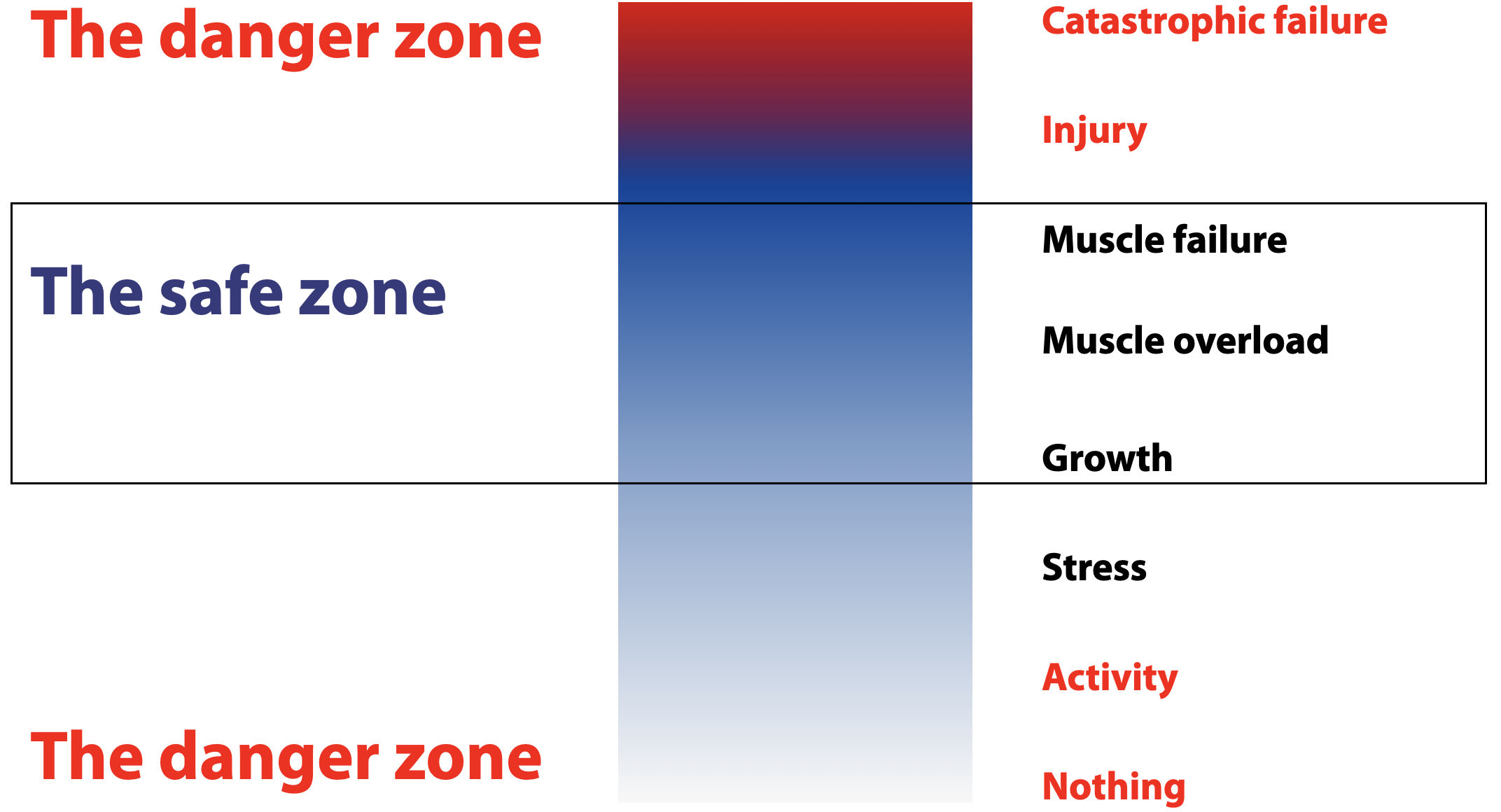
Everything is medicalized. You can get off the blood-pressure medication and reduce your A1c and your risk of heart disease by exercising. More exercise is better. Harder exercise is better. Pretending to exercise is not better. I show this slide to help people understand where the real risks are:
More than half of all doctors are out of date and routinely prescribe what big drug companies want them to prescribe. Why? Because patients would rather have medicine to lower blood pressure than do any exercise. They want drugs for everything, so that’s what doctors give them. Many common drugs and treatments don’t work, but some do. Only 15 percent of doctors are statistically literate — the rest can't pass a simple biostatistics quiz.
Outdated Practices & Ineffective Care. Studies show many medical practices are simply out of date and provide little to no benefit to patients, though many make money for doctors. One in eight studies leading to common medical recommendations has already been shown to be ineffective, yet doctors keep prescribing them. Only about 50 percent of doctors consistently follow current evidence. Fewer than 40 percent of doctors recommend exercise, because fewer than 40 percent of doctors exercise regularly themselves. Many surgeries (e.g., spinal fusions, stents) show no benefit over placebo, yet remain common.
Too many drugs are overprescribed. Here’s a short top-ten list:
Proton Pump Inhibitors (e.g., Omeprazole): For GERD; long-term use (>8 weeks) often lacks benefit, increases risks of kidney disease, fractures.
Antidepressants (e.g., Sertraline): For mild/subsyndromal depression; 50% of patients see no benefit, with risks of emotional blunting, sexual dysfunction.
Levothyroxine For subclinical hypothyroidism; no clear benefit in mild cases (TSH <10 mIU/L), yet widely prescribed, risking overtreatment.
Benzodiazepines (e.g., Lorazepam): For anxiety/insomnia; long-term use ineffective, increases fall risk (elderly) and dependence. ~30% of older adults overprescribed.
Antipsychotics (e.g., Risperidone): Off-label for dementia behavior; no consistent benefit, increases mortality risk in elderly (1–2% higher).
Bisphosphonates (Fosamax, Boniva, Actonel): For osteoporosis; long-term use (>5 years) may cause jaw osteonecrosis (1/10,000–100,000 risk), atypical femur fractures. Does not grow bone but prevents bone loss in an unhealthy way.
Antihypertensives (e.g., Lisinopril, Hydrochlorothiazide): no clear benefit in low-risk patients, risks hypotension, falls in elderly, and exercise replaces most.
Metformin For prediabetes or off-label (e.g., PCOS); minimal benefit vs. lifestyle changes (26% reduced diabetes incidence), risks GI issues, lactic acidosis (rare). Changing diet and exercise do the job better.
Statins (e.g., Atorvastatin): For low-risk patients, 20–30% see no cardiovascular event prevention (NNT 217 for heart attacks), with risks of muscle pain, diabetes.
NSAIDs (e.g., Ibuprofen, aspirin): For chronic pain; long-term use risks GI bleeding, kidney damage with minimal benefit over non-drug therapies.
Anticholinergics (e.g., Oxybutynin): For overactive bladder; marginal benefit in elderly, increases cognitive decline risk.
Gabapentinoids (e.g., Gabapentin): For chronic pain; limited efficacy for non-neuropathic pain, risks sedation, dizziness.
Half of all medical tests are unnecessary. We spend $200 billion a year on routine checkups that do nothing but make money for doctors. On the other hand, the new “functional medicine” people love to order tons of tests, saying “We check over 150 biomarkers.” Testing that many things is going to show some number or other is low or high, and that’s when the drugs and treatments start. It’s now fashionable to offer full-body scans that just make people worried about some little dark spot on a scan that later turns out to be nothing important. In many cases, the cure is worse than the disease.
People are going the wrong direction. They are gaining weight and losing muscle. I ask “How many people here can get up out of a chair without using your hands?” Usually about half the people can do that. Then I ask “How many of you would like to be able to do that in five years?” They hadn’t thought about that. Half of them won’t be able to. The less strength you have, the more limited your options.

About 60 percent of Americans in their 70s can get up without hands, but only about 35 percent can do so after age 80.
Lack of equipment. More than half of all senior-care facilities don’t really have any equipment at all. They have a few bands and dumbbells in a box. The staff aren’t trained properly. There is no program, there are just some activities that look like people are moving - gentle yoga, some pool exercises, some stretching. If these programs worked, people would not be gaining weight, but they are gaining weight. They are not getting stronger. Facilities with a gym have a fairly standard gym that isn’t geared to promoting strength and conditioning for older people. Facility owners have no idea what to install, so they put in some machines that look good on a sales tour or that are designed for rehab. I know one building where all the equipment has to be black, so the gym looks good in photos. A perfect example is that every gym should have parallel railings and wedges and benches so people can practice squatting and getting back up — this is almost nonexistent.
No ping pong. This is a disaster. Ping pong is one of the things older people can do to maintain and even improve hand-eye coordination. Yet management does not prioritize this or thinks it may be too dangerous. Ping pong helps keep people safe, because it develops reflexes that help prevent falls. They should have competitions, leader boards, and tournaments around the city. There should be state, regional, and national championships. People should be excited to improve their ping-pong skills and want to improve their rankings. All the other stuff is too slow.
Lack of motivation. People don’t use the gyms or move much, and instructors aren’t there to push them. People don’t have projects or goals, they have activities. They look forward to birthday parties rather than competitions or fitness goals. Sir Rod Stewart is now 81. He runs 100 meters in 19 seconds, and he has a goal of 17 seconds. How many people are that motivated at his age?

At age 81, Rod Stewart can run 100m in 19 seconds.
Noise in the longevity channel. Now there are billions of dollars pouring into longevity, but most of the money is going toward 1) exotic drugs that have never been shown to extend life in humans, and 2) exotic expensive treatments for rich people that are highly medicalized and do not provide longevity. Examples:
Canyon Ranch offers a 4-day, $20,000 “longevity” program that gives wealthy people a lot of attention, too many medical tests, and no lifestyle changes.
Equinox is launching a $40,000 per year longevity program. They are partnering with Function Health to measure too many things and pay too much attention to the medical side of longevity. It’s probably the first viable program I’ve seen that will help improve longevity, because they will focus on fitness. But will they have the programs I advocate, especially hormones and bone-building? Probably not. It seems aimed at people in their 40s and 50s. I hope it goes well — we need more awareness of fitness and less medicalization for longevity.
Blue Zones Center Miami is an ultra-exclusive, high-end medical treatment center designed to suck money out of rich people. No longevity will come of this. It may help catch a few cancers early, at the expense of many false positives and unnecessary treatments. I hope it fails miserably and bankrupts its investors.
How to fix this?
In my view, this is a crisis, because it is so preventable and probably costs less than what we’re doing now. Senior-living facilities are giving the market what it wants. The root problem is that there’s very little demand for prevention. But that can change. There are three things we should do immediately:
Competitive ping pong for every senior community. It doesn’t matter what the income level is. Ping pong is not difficult or expensive to set up, and a program is not that hard to put together. Residents need training, leaderboards, competitions, championships, and recognition. There should be dominant-hand games as well as non-dominant-hand competition. There is no excuse not to do this immediately.

Start longevity programs in each retirement community. These will be aimed at about 20 percent of residents who learn that they have a choice. They want a program, want to lose weight, want to get stronger, and want to increase healthspan. They need support. They would pay extra for a daily program that gives them individual consultation, individual fitness coaching, and a group class. This would take place every morning from 9am to noon or in the afternoons from 2-5pm (so the coach can go to another facility on the same day). The rest of the time, they are on their own, but they have assignments to do, goals to achieve, progress to track, and they wear their A1c badge, so everyone in the community agrees to support them in improving their health and reducing dependence on doctors. I propose to provide that program as an outsourced contractor service.
Start a few longevity-themed pilot projects. A few dozen senior communities around the country should commit to starting a program as I just described, with the goal of phasing that program in 100 percent, so that community becomes the longevity-focused community for its metro area. This will involve a completely different kind of gym, menu, even stairways. I’d like to see half a dozen pilot programs get going on this in 2026.
In the long run
Over the next ten years, senior living will start to shift significantly, not just because we know more what works but because future seniors are going to demand it. I have written a separate essay on the senior-living center of the future.
Cities like Miami Beach are now creating “Blue Zones” that they hope will attract people for the new healthy lifestyle they want to create. These cities have become victims of Dan Buettner, who coined the term blue zone and is now using it as a marketing tool to make money. He charges a huge amount of money to make these gorgeous reports that are excellent sales tools. There’s a lot of value here, because so many cities are in need of attention. As I have written to the people of Miami Beach: “Many good things will come of this, but longevity is not one of them.”
I would also like to talk with apartment-building developers, because they could offer longevity gyms and longevity programs that will attract buyers and renters to a more healthy and fitness-oriented lifestyle. A luxury condo building with a longevity program and specially designed gym will stand out among all the buildings with Euro-kitchens and floor-to-ceiling windows. I have a full business plan for this and can build the longevity gym to suit and run the program for any developer.

Want to work with me?
I believe I can create the disruptive category-leader company in longevity, because I’m actually focusing on health and longevity rather than medical tourism and pampering. But it takes more than I’m doing now. It takes a team. Here’s what I’m looking for:
Marketing. People pay for what they want, not what they need. Most people in their 60s would rather take a vacation to Vegas than invest in their own health. I think more women are concerned about their hair than about hormone replacement therapy (which would help improve their hair a lot). I’m surprised how little people care about their own health and how most people’s plan is to put it off until something catastrophic happens, then let the doctors deal with it. About 3 percent of the population is very fitness aware and already working on longevity, and 75 percent are passing up opportunities to become more healthy every day. That leaves roughly ten percent of people who can afford and would be open to extending their healthspan. These are my customers. I can get them, I just need to try more things and find what works. I want to do events, funnels, direct outreach, Instagram, Twitter, partnerships, institutional contracting, and more. Want to help? Get in touch.
Connections to investors. I hope to raise $250,000 from accredited investors to build all the funnels, online events, and client-acquisition systems. As we say in business, sales solves most problems. With more money I’ll focus on more sales, which will let me continue to hire, build, and scale. If you know any accredited investor who would like to talk with me, please introduce us.
Consultants in various markets. I’m looking for people in San Diego, Los Angeles, San Fernando Valley, Santa Barbara, Austin, and possibly Phoenix. These would be people I train to work with clients in senior communities in those metro areas. This is not online, this is going to communities to work with people 60 and up.
Contacts of corporate wellness directors at Vi Living, Atria, Leisure Care, Sunrise, Five Star, Ritz Carlton residences, W residences, Four Seasons residences, Miraval, and others.
Contacts at luxury building developers (condos, rentals) like Bosa Development and others.
If this is your first time here, go to the Facts page or explore the blog.
How Much Protein Do You Need?

I would summarize it like this for almost everyone:
0.8 gram/pound daily for most normal people.
1 gram/pound for hard core bodybuilders and hypertrophy.
More has no effect on building muscle.
Vegans probably need more just to make up protein quality.
People on ketogenic diets may want more, to stay in ketosis.
Less is probably suboptimal.
For muscle growth, studies show that 0.7–1.0 g/lb of protein daily maximizes muscle protein synthesis. A 2018 meta-analysis found that gains in fat-free mass begin to plateau around 0.7 g/lb, with little added benefit beyond 1.0 g/lb for those maintaining their weight (energy balance). For bodybuilders training intensely, 0.8 g/lb is typically the upper limit for body composition improvements. Beyond this, extra protein is often used for energy or stored as fat, not muscle.
For bodybuilders in a caloric deficit (e.g., cutting for weight loss before competition), higher intakes of 1–1.3 g/lb help preserve lean muscle mass, especially in leaner or advanced competitors. A 2020 study noted that while 0.6 g/lb supports lean mass gains, intakes above 0.7 g/lb offer diminishing returns for hypertrophy unless you’re trying to catch up from a deficit. For older adults, 0.7 g/lb helps prevent age-related muscle loss (sarcopenia) when combined with resistance training. And it probably helps to increase that by 0.1 g/lb for every decade over 70. So the general guidelines now are 0.7 to 1 g/lb. Strict vegetarians probably need more, to compensate for the lack of certain amino acids in many foods.
What about health risks? Some people are concerned that high protein harms kidneys or bones in healthy people. A 2019 analysis of NHANES data showed no kidney damage at intakes up to 0.6 g/lb, and a meta-analysis found that protein above 0.7 g/lb slightly increases kidney filtration without harm. High-protein diets also improve calcium absorption, potentially lowering fracture risk. However, very high intakes (>1.8 g/lb) may cause digestive discomfort, as seen in a recent study of elite cyclists. Some studies suggest high animal protein could raise cancer risk in specific groups, but this doesn’t broadly apply to active, healthy adults.
How to get enough protein
A woman who weighs 120 pounds should try to get 120 grams of protein per day. That would be 30 grams per meal three times per day, plus a protein shake or yoghurt separately. This list gives combinations of foods that add to 30 grams:
1 large chicken breast (3oz, 26g protein) + ½ cup Greek yogurt (plain, non-fat, 5g protein)
2 large eggs (12g protein) + 3oz salmon (23g protein)
1 cup cooked lentils (18g protein) + ½ cup cottage cheese (low-fat, 14g protein)
3oz turkey breast (25g protein) + ½ cup edamame (5g protein)
1 cup tofu (20g protein) + 1 cup cooked quinoa (8g protein)
3oz chicken breast (26g protein) + 1 large egg (6g protein)
½ cup Greek yogurt (plain, non-fat, 10g protein) + 3oz salmon (23g protein)
3oz turkey breast (25g protein) + ½ cup cooked lentils (5g protein)
½ cup cottage cheese (low-fat, 14g protein) + 1 cup tofu (10g protein) + ½ cup quinoa (4g protein)
2 large eggs (12g protein) + ½ cup edamame (5g protein) + 3oz chicken breast (13g protein, ~1.5oz portion)
In addition, one of these will help top you up:


For someone who weighs 160 pounds, you want 40 grams of protein four times per day. Here are some suggestions:
1 large chicken breast (4oz, 35g protein) + 1 large egg (6g protein)
3oz salmon (23g protein) + ½ cup cottage cheese (low-fat, 14g protein) + 1 large egg (6g protein)
1 cup cooked lentils (18g protein) + 3oz turkey breast (25g protein)
3oz chicken breast (26g protein) + 1 cup Greek yogurt (plain, non-fat, 15g protein)
Vegan Option: 1 cup tofu (20g protein) + 1 cup cooked quinoa (8g protein) + ¾ cup cooked black beans (7g protein) + ½ cup edamame (5g protein)
3oz turkey breast (25g protein) + ½ cup edamame (5g protein) + 1 cup Greek yogurt (plain, non-fat, 10g protein)
2 large eggs (12g protein) + 3oz chicken breast (26g protein) + ½ cup cooked lentils (5g protein)
3oz salmon (23g protein) + ½ cup cottage cheese (low-fat, 14g protein) + ½ cup quinoa (4g protein)
1 cup tofu (20g protein) + 3oz turkey breast (25g protein)
3oz chicken breast (26g protein) + ½ cup edamame (5g protein) + ½ cup cottage cheese (low-fat, 7g protein)
And include one of these at some point:


For bigger people who weigh 200 pounds, you’re shooting for 50 grams times four:
1.5 large chicken breasts (5oz, 43g protein) + 1 large egg (6g protein) + ½ cup Greek yogurt (plain, non-fat, 5g protein)
4oz salmon (31g protein) + ¾ cup cottage cheese (low-fat, 21g protein)
1 cup cooked lentils (18g protein) + 4oz turkey breast (34g protein)
4oz chicken breast (35g protein) + 1 cup Greek yogurt (plain, non-fat, 15g protein)
Vegan Option: 1.5 cups tofu (30g protein) + 1 cup cooked quinoa (8g protein) + ¾ cup cooked black beans (7g protein) + ½ cup edamame (5g protein)
4oz turkey breast (34g protein) + ¾ cup edamame (8g protein) + ½ cup Greek yogurt (plain, non-fat, 8g protein)
3 large eggs (18g protein) + 3oz chicken breast (26g protein) + ½ cup cooked lentils (5g protein)
4oz salmon (31g protein) + ¾ cup cottage cheese (low-fat, 21g protein)
1.5 cups tofu (30g protein) + 3oz turkey breast (25g protein)
4oz chicken breast (35g protein) + ¾ cup edamame (8g protein) + ½ cup cottage cheese (low-fat, 7g protein)
Structured aminos
I also have all my clients taking structured amino pills, which give you about a 30-gram equivalent by taking 3 pills 3 times a day (bigger people can take 4x3):

Summary
All together, it’s very possible to get around 1 gram per day, and that’s probably about right for most people. I tell my clients: try for 1 gram per pound of ideal body weight every day. You won’t always get that much. Don’t sweat it. Keep trying.
This conversation is great for longevity nerds and people who want to learn more details on protein requirements:
References:
Morton RW, et al. (2018). A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength.
Tagawa R, et al. (2020). Synergistic effect of increased protein intake and resistance exercise.
Jäger R, et al. (2017). International Society of Sports Nutrition Position Stand: protein and exercise.
Devries MC, et al. (2019). Changes in kidney function do not differ between healthy adults consuming higher- compared with lower- or normal-protein diets.
If you’re new here, explore other blog posts or go to the big longevity page.
How to lose a lot of weight not in a hurry

John, a 50-year-old man with a cherubic smile, nodded at me on the Zoom screen and said hello. It was clear from the first moment I saw him why he was talking with me. At 5’10” and 350 pounds, his goal was to get down to 200 pounds—a weight he hasn’t seen since his 20s. Six months ago, his doctor told him he’s probably a few months away from having to inject insulin, and that woke him up. He had gotten used to being heavy ever since high school, but now, he said, he was going to finally make a change.
John came with a plan: start with Ozempic, a medication he’d read could melt pounds away, then ease off later with diet and exercise. “I think this will get me going,” he said, his voice hopeful but hesitant. “I’ll lose the weight first, then you’ll help me put together a diet and exercise plan. Within 18 months, I’ll be in good shape and I’ll have tapered off the Ozempic.”
“Got it,” I said. “Before we go there, let’s look at all your options.”
Fasting
Fasting is a debt-based approach to losing weight. When you lose fat, you don’t lose any fat cells. The fat cells you have get skinnier, and they want the weight back. Fasting also loses muscle, which is hard to get back. You never want to lose muscle if you don’t have to. Since fasting is not a lifestyle change — it puts your body into emergency mode — it isn’t sustainable. While it may help lose weight, it doesn’t help keep the weight off, and keeping the weight off is 2/3 of the effort. Fasting doesn’t produce permanent weight loss; it kicks the can down the road rather than doing it right from the start.
Semaglutide
Ozempic and Wegovy are the same drug. It’s a GLP-1 medication that curbs appetite and slows digestion, helping people lose weight—potentially 40–60 pounds in a year for someone like John. It also lowers insulin resistance and cuts heart-disease risk by about 20 percent. It sounds like a way to jump-start his journey, and even Peter Attia has admitted it could work for people like John.
Essentially, the drugs mimic fasting. They force weight loss but incur a debt that must be repaid later. Many people are now going toward Mounjaro, which includes a second method of action and helps people lose more weight. Both cost around $1200 per month.
These drugs are not your friend. They are like a devil you make a deal with, and the devil always wins. You must keep taking it forever — at the same high price per year — or the weight comes roaring back, often replacing muscle with fat, leaving people worse off. People love the “honeymoon period,” where the weight magically disappears, but then they are left in a state where nothing tastes good and they must keep paying to not go back the way they were before.
In just a few years Semaglutide is already a $25 billion industry, because it has about the best business model any drug company could ever dream of: fast, superficial results and customers who become fully dependent, paying monthly rent forever.
John plans to taper off and rely on diet and exercise, but studies show that’s a risky bet. After Ozempic, John would need to master the same diet and exercise habits he’s struggled with for years, but now with more cravings and a more ferocious headwind — he’ll be working against the drug rather than his own body. At 50, with a history of skipping exercise, there’s no evidence he can easily “pay back” this loan by suddenly becoming a different person.
Surgery
Gastric bypass is likely John’s best bet to lose 150 pounds and keep most of it off. The roux-en-Y procedure creates a small stomach pouch the size of an egg and reroutes the digestive system, so he eats less, feels less hungry, and absorbs fewer calories. For John, this could mean losing 90–120 pounds in two years with a reasonable hope of keeping it off. It reduces insulin resistance immediately and eases joint pain, helping him move more at 50. But it requires tiny, protein-packed meals and regular exercise forever—habits John’s never stuck with.
Sleeve gastrectomy removes most of the stomach, leaving a small tube that holds less food and cuts hunger. It’s simpler but less effective than bypass, and some regain weight without sticking to small meals and exercise.
The gastric band, or lap-band, puts a tight band around the stomach to limit food intake, adjustable by a doctor. It’s the least invasive, but John might only lose 35–70 pounds, and many patients need the band removed later.
The best option
“John,” I explained, “both the drug and fasting are nonstarters. If you’re going to do one of those, at least fasting is a lot cheaper, but both will give the same result — weight loss followed by weight gain. This is not how you start your permanent weight-loss journey.”
I recommended he start the ketogenic diet and exercise program now, get into ketosis and the gym, start with a serious commitment to six hours of cardio per week plus stretching and movement, and see where we are in six months. We can assess our further options at that time.
It wasn’t exactly what he wanted to hear — he’d been imagining getting compliments from all his friends on losing weight so quickly. But my words sunk in. John didn’t need to be told that planning to exercise was very different from actually exercising, managing the schedule, building the habits, wanting to do the work every day rather than looking for excuses. But he did need to hear that it was the right next step.
The first three months
The most important part of the plan is getting into ketosis and exercising 8-10 hours a week. If John can’t do that, nothing is going to work. He’s never been in ketosis. He’s never exercised regularly. This has to be step one, or there will never be a step two.
See a primary-care doctor for tests (blood sugar, cholesterol, thyroid) and clearance for exercise, given pre-diabetes and joint issues. Discuss bypass eligibility (BMI >40 qualifies) with a bariatric surgeon for future planning and insurance coverage.
Have a coach. A coach will keep him accountable. You don’t want to give your coach a list of excuses why you weren’t able to work out three times last week — that’s not going to cut it. Make agreements and keep them.
Keto diet
Plan to get into ketosis and stay there. Get the How Not to Get Sick Cookbook and find other resources. Don’t wing it.
Focus on protein (80–100g/day): eggs, grilled chicken, fish, Greek yogurt, protein shakes.
Add fiber: 2–3 cups vegetables (spinach, broccoli), ½ cup whole grains (quinoa, brown rice).
Zero alcohol. Don’t drink calories unless it’s a whey-protein shake. Start drinking more water.
Zero sugar. Substitute alulose if needed.
Cut all carbs: No bread, muffins, grains, snacks, soda, fast food, or sweets.

Examples:
Breakfast: Greek yogurt with alulose, or eggs and strip steak
Lunch: chicken salad, olive oil dressing
Dinner: baked or grilled fish, green beans, olives
Snacks: nuts, cheese, keto snacks
Evening snack: high-protein yoghurt
One meal a week, give yourself a reward without losing ketosis. It could be buckwheat pancakes with alulose syrup or eggs benedict with whole-wheat english muffin.
Exercise 30-minutes per day
Walking doesn’t count. Work out as hard as you are able. Treadmill, stairmaster, elliptical, bike, rower - whatever you will do for 30 minutes, work up a sweat, and count the number of calories expended. Start with 300 calories per session and go up eventually to 600.
Within two months, try to be at one hour per day and 600 - 800 calories. Start a movement, yoga, or stretching class that you have to go to twice a week. Not so much for the results but for the habit.
Support
Make sure you are in ketosis and stay there. Your breath should smell like acetone (nail-polish remover). Don’t break ketosis.
There will be setbacks. Come up with a plan for making yourself work out daily. Specify what happens if you don’t. Get a buddy or someone to keep you accountable. Don’t make bad decisions based on not feeling like it. Find a way to keep your commitment. This is the hardest part, so build systems to get around your mood and feelings and justifications.
Don’t focus on how many pounds you lose! Focus on your ability to adopt and maintain your new routines and stay in ketosis. Don’t try to lose too many pounds too quickly - make sure you’re getting enough food daily to maintain your muscle mass.
Months 3–6: ramp up, don’t slide back
Build all your shopping routines. Manage all your work-out clothes and washing routines so everything is ready for going to the gym. Manage your schedule around your workouts. Join some classes and teams, commit to weekly runs or other activities with others in the same situation. Prioritize the workouts, so if something has to give it’s not the exercise.
Work on getting 7+ hours of sleep per night.
Identify sources of stress and manage them. Remove external stress as much as possible. Seek any additional resources you need.
Drink even more water.
Plan a trip that involves a big hike or camping trip or bike ride where you’ll be on your feet burning calories 8 hours a day for several days. There are hundreds of multi-day endurance events of all kinds happening around the country every year. A big trip takes planning, preparation, thinking more about diet, and coordinating with others toward a common goal. It brings people together who can support each other.
Work more on balance, stretching, movement. See Lee Weiland’s videos for inspiration.
Don’t focus on pounds lost! Don’t lose too many too quickly — make sure you’re eating a sustainable diet that prevents loss of muscle.
Six-month assessment
At this point, John’s mind should be in a better place to make a good decision. He should have researched the surgery options. We can decide whether to add surgery to his already good habits or continue building on the success so far. At this point, the most important thing is to not slide back, because the weight wants to come back.
The ketogenic diet should be doing half the work and the exercise the other half. If things are going well at this point, surgery in the next six months would give an added boost to what he’s doing already and help lock in gains.
Or not — it’s entirely possible to lose 150 pounds and keep it off, but it’s better in that case to move on to half-marathons, wilderness backpacking, distance swimming, extended bike road trips, endurance events, and other hard challenges. Are you ready to climb Mt Shasta now, John? Even if you go and don’t make the summit, you’ll have something to aim for next year.

Less money and better results than Wegovy or Ozempic.
Summary
While it’s possible for John to lose all 150 pounds on his own, there are other options. No amount of drugs or surgery is going to give John the body he really wants. Rather than paying rent to Eli Lilly, embracing his new athletic life will pay him dividends forever. It will lead him to meet new people, have amazing experiences, build his confidence by accomplishing hard missions, and feel great from head to toe. It may even land him another job that he could never have gotten without getting in shape.
John exhaled, nervous but nodding. It was time to actually start doing what he had been avoiding for his entire adult life. His road to losing 150 pounds won’t be quick—50 years of habits and a body that fights change make it a long journey. But a journey like this requires small steps at the beginning, not a giant leap.
Is Saturated Fat Still the Villain We Thought?

For decades, saturated fat—found in butter, red meat, and cheese—has been cast as a dietary demon, blamed for clogging arteries and triggering heart attacks. Public health campaigns urged us to swap steak for salads and butter for olive oil, promising longer, healthier lives. Yet, beginning with Dr Atkins in the late 1990s, it started to become clear that the low-fat/high-carbohydrate diet was not the answer for everyone. As heart disease remains the leading cause of death globally, a growing chorus of researchers, doctors, and journalists questions whether saturated fat deserves its reputation as a silent killer. The science, they argue, is less conclusive than we’ve been told, and the answer depends on who you are, what you eat, and how your body responds.
To unravel this debate, I’ll use two sources: experts and metastudies.
The experts
First, let’s look at the views of seven key voices shaping the conversation:
Gary Taubes: the keto warrior
Gary Taubes, author of Good Calories, Bad Calories and The Case for Keto, sees saturated fat as a scapegoat in a misguided war on fat. He argues that carbohydrates, not fats, drive heart disease by spiking insulin, which promotes fat storage and inflammation. “The low-fat mantra failed us,” Taubes told The Guardian in 2021. “Heart disease rates didn’t plummet when we ditched butter for bread.”
Taubes points to historical data and observational studies suggesting no clear link between saturated fat and heart disease. A 2010 American Journal of Clinical Nutrition meta-analysis found no significant association between saturated fat intake and cardiovascular disease (CVD) risk in 350,000 people. He also cites the rise in obesity and diabetes since the 1980s low-fat push as evidence that carbs are the real problem.
Taubes advocates unrestricted saturated fat intake within a ketogenic diet (<50 grams carbs/day), favoring butter, beef, and eggs over processed carbs. He claims this approach cuts CVD risk by 20–30% by reducing insulin-driven inflammation, especially for those with obesity or diabetes. For older adults (60–90), he sees keto as a way to reverse metabolic issues, potentially adding 3–5 years to life.
Critics, including a 2017 Cochrane Review, note that reducing saturated fat to <10% of calories lowers CVD events by 17%. Taubes’ dismissal of LDL cholesterol’s role in heart disease clashes with mainstream cardiology.
Ben Bikman: insulin resistance as the true enemy
Dr Ben Bikman, a biomedical scientist and author of Why We Get Sick, zeroes in on insulin resistance as the root of heart disease. “High insulin levels damage arteries and fuel plaque buildup,” he explained in a 2022 podcast. Keto diets, high in saturated fat but low in carbs, reverse this by keeping insulin low, he says.
Bikman cites studies like a 2021 Journal of Clinical Lipidology trial showing keto diets reduce triglycerides (15–25%) and improve blood sugar (HbA1c drops ~0.7–1.2%), cutting CVD risk factors by 15–20%. He argues saturated fat’s impact on LDL is less concerning in a low-insulin state, pointing to a 2021 American Journal of Clinical Nutrition study showing whole-food saturated fats (e.g., eggs) don’t clearly raise CVD risk.
Bikman supports saturated fat from whole foods (e.g., meat, dairy) within a keto diet, aiming for <50 grams carbs/day. He estimates a 15–25% CVD risk reduction for insulin-resistant people. For older adults, he stresses adequate protein (1.2–1.6 g/kg body weight) to prevent muscle loss, which could indirectly raise CVD risk by 5–10%.
However, a 2023 BMJ meta-analysis linked low-carb, high-fat diets to a 10–15% higher CVD risk over decades, suggesting long-term risks from LDL elevations Bikman downplays.
Peter Attia: precision over dogma
Dr Peter Attia, a physician, author of Outlive, and host of The Peter Attia Drive, once championed keto but now takes a nuanced view. “Keto works for some, but it’s not a one-size-fits-all,” he said in a 2021 podcast. He focuses on individual responses, using advanced lipid tests like apolipoprotein B (apoB) to gauge heart disease risk.
Attia acknowledges keto’s benefits: a 2021 Nutrients trial showed it reduces weight (5–10%) and triglycerides (10–20%), potentially lowering CVD risk by 10–20% in insulin-resistant people. But he warns that 30–50% of keto dieters see LDL spikes, increasing CVD risk by 10–15% if apoB rises (Journal of the American College of Cardiology, 2022). He prefers monounsaturated fats (e.g., olive oil) over saturated fats.
Attia advises limiting saturated fat (<20 grams/day) and monitoring apoB. He supports keto for diabetes or obesity but suggests cycling off after 3–6 months. For older adults, he’s cautious, citing risks of muscle loss and low fiber, which could raise CVD risk by 5–10%. He estimates a neutral to 10% CVD risk reduction with proper management.
Attia is a concierge doctor to billionaires. His reliance on advanced testing may be inaccessible, and long-term keto mortality data are lacking, as noted in a 2018 Lancet Public Health study showing low-carb diets increase mortality by 15–20% over 25 years.
Mark Hyman: A healthier keto diet
Dr Mark Hyman, a functional medicine physician and author of many books on nutrition, views keto as a short-term tool for conditions like diabetes or obesity, not a lifelong diet. “Done right, keto can reset your metabolism,” he wrote in The Pegan Diet. He emphasizes whole foods and a “healthy keto” with low-carb vegetables and nutrient-dense fats.
Hyman cites a 2018 Cleveland Clinic study where keto improved 22 of 26 CVD risk factors, including inflammation (C-reactive protein drops 10–20%) and HDL (5–10% rise), potentially cutting CVD risk by 15–20%. He’s less worried about saturated fat from whole foods like eggs but urges moderation (10–15% of calories) to avoid LDL spikes.
Hyman suggests a cyclical keto (e.g., 5 days on, 2 days off) with olive oil, avocados, and fish over butter or red meat. He estimates a 15–20% CVD risk reduction short-term for metabolic issues. For older adults, he prefers a Mediterranean-style keto to avoid nutrient deficiencies, which could raise CVD risk by 5–10%.
Hyman’s optimism lacks long-term mortality data. A 2023 BMJ study suggests low-carb, high-fat diets increase CVD risk by 10–15% over time, challenging his long-term claims.
Thomas Dayspring: the lipidologist’s warning
Dr Thomas Dayspring, a lipidologist, is laser-focused on apoB, the protein in LDL particles that drives atherosclerosis. “ApoB is the best predictor of heart disease risk,” he told The Peter Attia Drive in 2025. He sees keto’s high saturated fat content as a potential problem, elevating apoB in 30–40% of people.
Dayspring acknowledges keto’s short-term benefits: a 2021 Nutrients trial showed it reduces metabolic syndrome markers by 15–20%, potentially lowering CVD events. But he warns that apoB spikes increase CVD risk by 15–25% (Journal of Clinical Lipidology, 2019), potentially shortening life by 3–5 years. He recommends replacing saturated fats with olive oil or fish.
Dayspring advises capping saturated fat at 10–15% of calories (~20–30 grams/day) and monitoring apoB weekly. He supports keto for insulin resistance but prefers Mediterranean diets for long-term CVD prevention (20–30% risk reduction). For older adults, he’s skeptical, citing risks of sarcopenia and low fiber.
Dayspring’s focus on apoB is evidence-based, but his caution about keto may overlook individual variations where apoB remains stable, as noted in some keto trials.
Mario Kratz: the dairy defender
Dr Mario Kratz, a nutrition researcher in Austria (formerly at the University of Washington), studies dairy fats and their complex effects on health. “Saturated fat isn’t a single villain,” he told Nutrition Reviews in 2020. His work suggests dairy fats (e.g., in cheese, yogurt) may not harm heart health as much as once thought due to their unique fatty acid profiles and nutrient matrix.
Kratz cites a 2021 American Journal of Clinical Nutrition study showing dairy fats don’t significantly raise CVD risk, unlike red meat fats. He argues that foods like yogurt may even lower CVD risk by 5–10% due to probiotics and calcium. However, he agrees with mainstream guidelines that high saturated fat intake (>10% of calories) increases LDL, raising CVD risk by 10–15% (Circulation, 2020).
Kratz supports moderate saturated fat (7–10% of calories) from dairy but advises limiting red meat and tropical oils. He recommends whole-fat yogurt and cheese within a balanced diet, estimating a neutral to 5% CVD risk reduction. For older adults, he sees dairy as a nutrient-dense option to combat frailty, potentially lowering CVD risk indirectly by 5–10%.
Kratz is one of the few keto proponents to acknowledge the risk of eating too much saturated fat. He advocates mixing nuts, avocado, fish, beans, lentils, and tofu into your diet to replace carbs with protein and healthy fats.
Tim Noakes, the saturated fat promoter
Dr. Tim Noakes, an Emeritus Professor at the University of Cape Town and a National Research Foundation A1-rated scientist, has significantly influenced nutrition discourse, particularly through his advocacy for low-carbohydrate, high-fat (LCHF) diets. His views on saturated fat and heart disease challenge conventional dietary guidelines, positioning him as a polarizing figure in medical and nutritional circles.
Noakes’s stance is that saturated fat does not cause heart disease, a view he has expressed in various forums. Noakes argues that excessive carbohydrate consumption, particularly refined sugars and starches, is the primary dietary factor contributing to heart disease. He has published several articles explaining why he believes sugar and carbohydrates are the leading causes of heart disease — via insulin resistance.
A good question to ask is: what do saturated fats replace? If they replace unsaturated fats in your diet (avocados, nuts, fatty fish), that could move some people toward a higher chance of heart disease. On the other hand, if they replace carbohydrates, that could be worse for many people. Insulin resistance contributes a lot to heart disease, so the pizza could be even worse for your heart than the steak.
The metastudies
Now, let’s look at the evidence ourselves. Metastudies are critical, because they combine many trials into one view. They are usually done by statisticians and therefore help shed light on which studies are higher quality. Not all metastudies are valuable, but most are. More recent metastudies are better than older metastudies. In general, metastudies before 2016 are not worth spending time on. In most cases, you want metastudies that look at endpoints like heart attacks, stroke, and death, rather than biomarkers like cholesterol or triglycerides in the blood.
One of the problems with any studies of diet and outcomes is that it’s extremely expensive to control all the factors, so researchers generally use epidemiological studies, which are far less reliable. Most metastudies, therefore, concentrate on randomly controlled trials. Here are some of the most recent, in chronological order …
Supports the idea that saturated fat causes heart disease:
Reduction in saturated fat intake for cardiovascular disease, 2020
Conclusion: Reducing saturated fat intake for at least two years causes a potentially important reduction in combined cardiovascular events. Replacing the energy from saturated fat with polyunsaturated fat or carbohydrate appear to be useful strategies, while effects of replacement with monounsaturated fat are unclear. The reduction in combined cardiovascular events resulting from reducing saturated fat did not alter by study duration, sex or baseline level of cardiovascular risk, but greater reduction in saturated fat caused greater reductions in cardiovascular events.
Does not support the idea that saturated fat causes heart disease:
Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations: JACC State-of-the-Art Review, 2020.
Conclusion: Most recent meta-analyses of randomized trials and observational studies found no beneficial effects of reducing SFA intake on cardiovascular disease (CVD) and total mortality, and instead found protective effects against stroke. Although SFAs increase low-density lipoprotein (LDL) cholesterol, in most individuals, this is not due to increasing levels of small, dense LDL particles, but rather larger LDL particles, which are much less strongly related to CVD risk. It is also apparent that the health effects of foods cannot be predicted by their content in any nutrient group without considering the overall macronutrient distribution. Whole-fat dairy, unprocessed meat, and dark chocolate are SFA-rich foods with a complex matrix that are not associated with increased risk of CVD. The totality of available evidence does not support further limiting the intake of such foods.
Supports the idea that saturated fat causes heart disease:
Association between dietary fat intake and mortality from all-causes, cardiovascular disease, and cancer: A systematic review and meta-analysis of prospective cohort studies, 2021.
Conclusion: Diets high in saturated fat were associated with higher mortality from all-causes, CVD, and cancer, whereas diets high in polyunsaturated fat were associated with lower mortality from all-causes, CVD, and cancer. Diets high in trans-fat were associated with higher mortality from all-causes and CVD. Diets high in monounsaturated fat were associated with lower all-cause mortality.
Does not support the idea that saturated fat causes heart disease:
Saturated fat: villain and bogeyman in the development of cardiovascular disease?, 2022
Findings from the studies reviewed in this paper indicate that the consumption of SFA is not significantly associated with CVD risk, events, or mortality. Based on the scientific evidence, there is no scientific ground to demonize SFA as a cause of CVD. SFA naturally occurring in nutrient-dense foods can be safely included in the diet. My problem with this study is it may have put too much emphasis on the PREDIMED trial, which in my view was very poorly done.
Supports the idea that saturated fat causes heart disease:
Red meat consumption, cardiovascular diseases, and diabetes: a systematic review and meta-analysis, 2023
Conclusion: Unprocessed and processed red meat consumption are both associated with higher risk of CVD, CVD subtypes, and diabetes, with a stronger association in western settings but no sex difference.
Does not support the idea that saturated fat causes heart disease:
Saturated Fat Restriction for Cardiovascular Disease Prevention: A Systematic Review and Meta-analysis of Randomized Controlled Trials, 2025.
Conclusion: The findings indicate that a reduction in saturated fats cannot be recommended at present to prevent cardiovascular diseases and mortality.
Conclusion?
Dr John Ioannidis from Stanford is one of the leaders of the meta-analysis movement. He teaches medical statistics and how to do good metastudies. While he hasn’t written specifically about saturated fat, it seems likely that Ioannidis would say the evidence linking saturated fat to heart disease is weak and largely based on flawed observational studies. He would call for more rigorous studies before making population-wide recommendations and warn against overconfidence in nutrition guidelines that rest on poor-quality data.
What should you eat?
The results are clear as mud: we have no idea what causes heart disease! And yet, heart disease kills more people than any other. More research is needed!
Still, we have to eat something. What should we eat?
In my view, the first thing we should all do is exercise more. From a diet perspective, the confusion could very likely come from the fact that researchers don’t take insulin resistance into account when they run trials, so that confusion makes its way through the system. I’m not a doctor, I’m not a professional researcher, so your reading of the above evidence may differ from mine, but here’s how I would summarize:
Processed meats are probably not ideal. Processed meats — bacon, hot dogs, salami, anything that comes in a can — probably aren’t as healthy as cooking fresh meat. I think all the experts would agree we should limit those to just treats, rather than part of a good diet.
For People with Insulin Resistance or Type 2 Diabetes: Maintain ketosis and watch your ApoB number. If it’s too high, reduce red meat and focus more on chicken, turkey, fish, beans, lentils, and tofu. Get plenty of fiber and fresh foods.
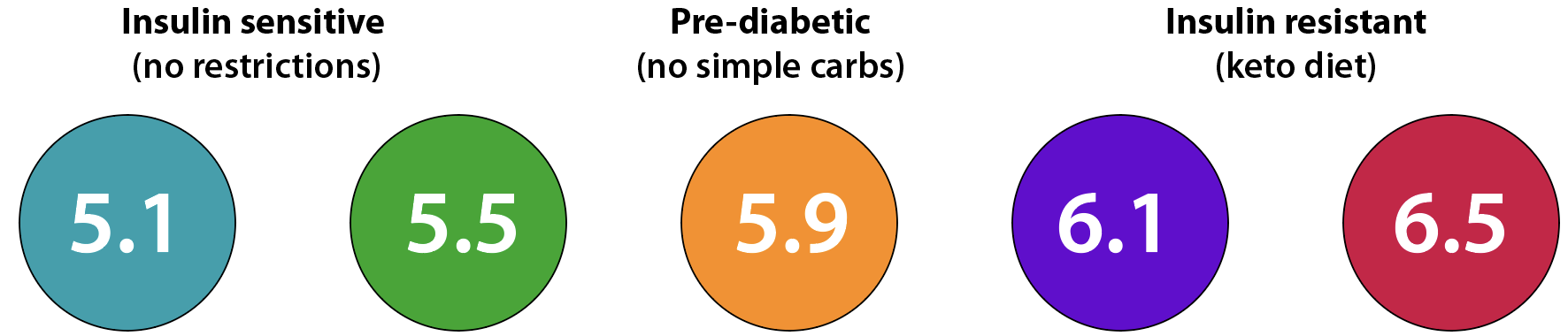
For Older Adults (60–90): Eat to modify your A1c number first. Below 5.9, you don’t need to be in ketosis, but you should limit sugars and carbohydrates until you’re under 5.7. Focus on getting enough protein — the older you are, the more protein you need. This population should eat between .8 and 1 gram of protein per pound of ideal body weight per day. Limit simple carbohydrates to once or twice a month. Get plenty of fiber and fresh foods.
For people overweight: Again, use your A1c number to guide you on your weight loss journey. See my weight-loss page for details.
For athletes: Carbs are critical. Most athletes should get 0.8 grams of protein per pound per day and use carbs to fuel your muscles. Don’t let your A1c number go above 5.6 — if it does, lower your glycemic load.
For vegetarians: Hyman’s cyclical, plant-rich keto and Kratz’s dairy-moderated diet align with your goals. Keep your A1c under 5.7 first. Use whey protein to help get enough and support muscle growth. Take some B vitamins to add insurance. And get plenty of fiber and fresh foods.
For vegans: veganism is not a healthy diet. I say that as someone who was vegan for 45 years and wrote one book on the benefits of being vegan. I plan to write more about what I have learned. If you care about your health, choose another option.
For people on a carnivore diet: We know almost nothing about this. Because it keeps people in ketosis, it’s good for losing weight. Is it a good long-term diet? My answer is that if your ApoB stays under 100, it might be, but by eliminating fiber from your diet, you’re going far outside the boundaries of what most scientists believe is healthy. You may not die of heart disease, but you may get cancer. You may also want to watch other factors, like iron, calcium, etc. Could you live on a carnivore diet and just take lots of cholesterol-lowering drugs? Who knows? No one knows the answer to that question.
Saturated fat doesn’t seem to be a universal villain, but it’s not yet clear that it’s harmless. Neither a fully plant-based nor a fully meat-based diet will support optimal health, but there are many good choices in between. In my view, your A1c number will tell you what you can and can’t eat, and your ApoB number will tell you how much saturated fat you should tolerate. Perhaps in another ten years, we’ll know more, but for the moment, we need to read the evidence critically and keep our minds open to the idea that we simply don’t know as much as we would like to know about saturated fats and heart disease.
Want to lose weight? Come to my weight-loss page.
Want to live 10-20 years longer? Learn the facts.
The benefits of more exercise

At 72, Maggie thought her best days were behind her. A retired librarian from Ohio, she’d spent years behind a desk, her only exercise the occasional stroll through her garden. Now, she had a diagnosis of osteopenia, she got tired going up stairs, her knees ached, and she worried about her heart—her father had passed from a heart attack at 68. But last year, Margaret’s daughter convinced her to join a local walking group. Five days a week, she laced up her sneakers for a 30-minute brisk walk with neighbors, chatting and laughing through the park. Within months, she felt stronger, sharper, and, to her surprise, happier. “I didn’t realize how much moving could change me,” she said. “I want to do more.”
Maggie started working with a trainer. In addition to walks, she started doing movement routines, lifting moderate weights, and rucking — hiking with a weight pack on her back. While that sounds extreme, she worked her way up slowly and avoided injury. Now at age 74, she feels stronger, more stable, and much less likely to fall and get hurt.
From moderate to more vigorous
Whether it’s a daily walk or an ambitious mix of running and weightlifting, movement delivers measurable benefits. Let’s explore two approaches: a moderate routine of 3.5 hours a week (like Margaret’s walks) versus an intensive 10-hour weekly mix of vigorous cardio and strength training. The science shows both can transform health, but the choice depends on your goals, fitness, and lifestyle.
The Easy Win: Moderate Exercise (3.5 Hours a Week)
Picture a week where you spend just 30 minutes a day, five days a week, walking briskly, cycling gently, or tending a garden. This moderate mix—3.5 hours total—fits easily into most schedules and delivers powerful results for older adults. Studies show it’s like a shield against major health threats. For Maggie, this routine got her out of her old, sedentary lifestyle. “I’m not out of breath climbing stairs anymore,” she says. “And I sleep better, too.” The beauty of moderate exercise is its accessibility. No gym membership or fancy gear is needed—just a pair of comfortable shoes and a commitment to move.
The Big Leap: Vigorous Mixed Exercise (10 Hours a Week)
Now imagine a more ambitious approach: 10 hours a week of intense exercise, split between running (or fast cycling) and heavy weightlifting. This vigorous mix—about 85 minutes a day, six days a week—is for those ready to push their limits, and Maggie was ready. “I wanted to stay strong, not just for me but for my grandkids,” she says. “I’m lifting heavier than I could have ever imagined!” The stronger she gets, the better and more unbreakable she feels. Her cardiologist was most impressed. “He said I’ve reversed my age by 20 years,” Maggie reported after a recent visit.
Moderate exercise or more intense?
Moderate exercise, like Maggies initial 3.5 hours of walking, is a low-risk, high-reward choice for most older adults. It’s easy to start, fits busy lives, and delivers solid protection against major health issues. But it’s not that much more to go from a moderate mixed exercise regime to a more vigorous mixed schedule, and it has huge benefits. The more intense approach shines for bone health and physical independence, thanks to weightlifting, while its cardio component gives an edge for heart and brain health. After two years, Maggie had transformed from a weak grandma to a strong member of her local rucking club, getting more and more of her friends to buy weight vests and come along on their hikes.
The health benefits range from reduced risk of heart attack to reduced risk of cancer, dementia, falls, fractures, depression, and more …

Anyone who isn’t exercising can benefit from starting. Moderate exercise carries little risk, while vigorous routines need careful planning—proper form for lifting and gradual increases in running intensity. Not only do you feel better, but you can stop taking various medications for hypertension, osteoporosis, and more. Women should be on a smart hormone replacement therapy to get the most benefit out of exercise.
Start with moderate walks, add a light weight vest, and add strength or cardio as you build confidence. Combining both, like 2–3 hours of walking plus 1–2 hours of lifting or jogging, can cover all bases.
Whether you’re strolling through a park or lifting weights at the gym, movement is medicine. For those 60 to 90, it’s not about chasing youth—it’s about living fully, with a stronger heart, sharper mind, and the energy to enjoy life. Check with your doctor, find an activity you love, and start moving.
Should you start HRT in your 70s or 80s?

Image created by ChatGPT
In 2002, the Women’s Health Initiative (WHI) announced findings suggesting Hormone Replacement Therapy (HRT) increased risks of breast cancer and heart disease, scaring many women away from it just as they hit menopause 20+ years ago. Those results were misleading, as they focused on older women using oral synthetic hormones, not safer modern options. Since then, extensive evidence, including WHI 2020 follow-up, 2022 Menopause meta-analyses, and 2024 Menopause Society studies, shows HRT—especially transdermal estrogen and micronized progesterone—is safe and beneficial for many, even those with a history of breast cancer or blood clots. This article, based on recent research, meta-analyses, and UpToDate, explains why it’s smart to consult a urologist or endocrinologist about HRT now, even if you never started.
If you’ve had breast cancer or a blood clot, you may have heard that hormone replacement therapy (HRT) is off-limits. The main reason for that is they gave both synthetic estrogen and synthetic progesterone in pill form, and it turned out that synthetic progesterone (progestin) really did cause more breast cancer in those 60+ women. However, dozens of studies, including the Women’s Health Initiative (WHI) 2020 follow-up and a 2022 Menopause meta-analysis, show that transdermal estrogen (patches or gels) and micronized oral progesterone can not only be safe and effective for many women with these histories, but they help prevent cancer as women age. HRT, which can include various methods of delivering estrogen (E), progesterone (P), and testosterone (T), can ease symptoms, protect health, prevent cancers, and improve quality of life. Even women who have had a hysterectomy should consider taking micronized progesterone for its other important benefits.
Common Benefits for Women in Their 70s and 80s
HRT relieves genitourinary symptoms of menopause, easing vaginal dryness and reducing recurrent urinary tract infections (UTIs), which can be life-threatening. Vaginal estrogen is highly beneficial for almost all post-menopausal women. Micronized oral progesterone supports uterine health by preventing endometrial hyperplasia (a cancer precursor). It also promotes better sleep for many women. Testosterone can boost energy and strength, enhancing vitality. Both estrogen and testosterone support building muscle and bone through resistance and impact exercises. The added muscle helps improve agility, lowering fall risk—the leading cause of death for women over 75. Transdermal estrogen and micronized progesterone lower stroke and blood clot risks by 20–30% compared to oral forms, and estrogen-only patches can reduce breast cancer risk, per WHI 2020 data.
Women in Their 70s: Specific Guidance
Unique Benefits: About 15% of women in their 70s have hot flashes, disrupting daily life. Systemic HRT (E, P, and possibly T) relieves hot flashes, improves sleep with progesterone’s calming effects, and boosts energy and strength with testosterone, per a 2024 Menopause Society study. HRT reduces sarcopenia (affecting 24% of women in this age group) and builds bone mass, enhancing mobility and preventing falls. For most women in their 70s, systemic HRT’s benefits—symptom relief, UTI prevention, uterine health, better sleep, energy, and fall reduction—often outweigh risks when carefully managed, per the 2022 Menopause Society Statement.
Depending on your cardiovascular profile, systemic HRT may slightly increase stroke or blood clot risks, but patches, gels, or micronized progesterone minimize these, with estrogen-only patches potentially lowering breast cancer risk (WHI, 2020). In most cases, women in their 70s get far more benefit from HRT than the risks they take going without it.
Women in Their 80s: Specific Guidance
Unique Benefits: Around 10% of women in their 80s have hot flashes, and genitourinary symptoms remain prevalent, increasing UTI risk. Vaginal estrogen effectively treats dryness and prevents UTIs. Systemic HRT may help severe symptoms, with progesterone aiding sleep and testosterone supporting energy and strength, but it’s less common due to higher risks from conditions like heart disease. HRT supports exercise to build bone and muscle, reducing sarcopenia (affecting 31% of women in this age group) and fall risk, per the 2024 Menopause Society study. Localized HRT (e.g., vaginal estrogen) is safer, but your doctor may still suggest trying an estrogen patch, because going without it may be even more risky.
Action Steps
Talk to Your Doctor: Explore E, P, and T, focusing on GSM, UTIs, sleep, energy, and mobility.
Read a good book ahead of time, like The New Menopause, by Mary Claire Haver, or Top Ten Reasons Why Your Hormones are Failing You, by Doug Lucas.
Discuss all options with your doctor. There’s very little risk in trying something for 3-6 months. Work with your doctor over this period to find a combination that may provide more benefit than the risk you’re taking now without HRT.
Take micronized progesterone if you possibly can, it has many important benefits. Some women don’t tolerate it, but most do after an initial adjustment period.
Don’t leave out the benefits of testosterone for women. If your doctor doesn’t understand the benefits, read up and get him/her to try a low dose and see how it goes.
All women over 50 should consider the use of vaginal estrogen creams, as I have outlined in a previous blog post.
Strength Train: Combine HRT with exercise to build bone and muscle to reduce risk of falls and fractures.
HRT may not be right for everyone, but all women in their 70s and 80s should consider their options. Vaginal creams offer safe relief for GSM and UTIs at any age, making them a great starting point. Hormone therapy can be very beneficial — learn about the newest research and talk with your doctor about reducing your risk through HRT.
Preventing Gym Injuries in Older Adults

Starting a new exercise routine can be exhilarating, but for older adults — especially former athletes — it’s crucial to approach it with caution. Small muscles, like those in the forearms and shoulders, are particularly vulnerable to overuse injuries such as tennis elbow, which can take months or even years to heal. The key to avoiding such injuries is not just caution but a deep understanding of one’s limits and a commitment to gradual progression far below your capabilities. Your body will take time to get used to the new regime. Give it a year, not a few weeks. A five percent gain in one year is far better than a 20-percent gain and a nagging injury.
The Vulnerability of Small Muscles
Small muscles, though less conspicuous than their larger counterparts like biceps or quads, play a critical role in joint stability and movement. Their smaller size, rare use, and higher tendon-to-muscle ratio make them susceptible to strain. For instance, the forearm extensors, involved in gripping exercises, can develop tennis elbow if overworked without adequate preparation. Do not attempt to build grip strength without an experienced instructor. Similarly, the rotator cuff muscles, essential for shoulder stability, risk strain during compound movements that aren’t carefully designed. According to an article in WebMD, overuse injuries such as tendonitis often affect these areas due to repetitive stress, with recovery potentially extending months or years. Older adults, with age-related declines in muscle mass, bone density, and flexibility, are particularly at risk, as studies from the National Center for Biotechnology Information (NCBI) show delayed and less efficient recovery from muscle damage.
One of the challenges with overuse injuries is that they often develop insidiously—you might not feel pain immediately after a workout, but over a few weeks, the cumulative effect of too much stress on your muscles and tendons can lead to an injury you immediately regret by the time you feel it. That’s why it’s crucial to follow a structured plan and not rely solely on how you feel in the moment. Just because you “haven’t been hurt yet” doesn’t mean you’re okay to keep going. By limiting the total number of reps per week for each muscle group and ensuring adequate rest, you can stay well under your injury threshold.
Grip strength
Most people hear how important grip strength is, so they buy several grip trainers on Amazon and start pumping them several times a day. That’s how you get tennis elbow that doesn’t heal for months and months.
For grip strength, grab a pair of light dumbbells, like 10 or 15 pounds, hold them down at your sides, and relax your grip, so the dumbbell is held very loosely toward the end of your fingers. Hold this for 30 seconds. It should be trivially easy. Do that 3 times in one day. Do that every three days to start, skipping two days in between. Then go up 5 pounds in each hand. Don’t even think of going to every other day during the first year. If you get to 15-20 pounds per hand three times in one day, three days a week — gradually — in the first year, you’re doing it about right. With that base after the first year, you can start moving into new territory.
If you want to do farmer carries, grab two 25-pound barbell plates and carry those with a full grip. If that’s too heavy, start with kettlebells or dumbbells and a full grip. Always do farmer carries with a straight spine and head held high. The biggest danger in farmer carries is loading and unloading, so start with less weight and build good form before moving up.
For a former athlete, this will be frustratingly slow. Be patient. Build your platform first.
Principles of Injury Prevention
For most people, warming up is critical: a 5–10-minute dynamic warm-up, such as arm circles or leg swings, increases blood flow and prepares muscles for exertion. Don’t just jump into it. Cooling down with static stretches, held for 20–30 seconds, aids recovery and reduces stiffness. Use gravity for stretches when possible. Gradual progression is equally vital; the “10% rule,” supported by EōS Fitness, suggests increasing workout intensity by no more than 10 percent weekly to allow tendons and ligaments to adapt. However, for older adults, especially those new to exercise, change that to ten percent monthly, max. Start light. Instead of lifting to failure or doing too many reps, begin with weights that allow you to perform 6-8 reps with perfect form but without straining. Stop well before your maximum — leave the hard work for later. Go until you feel a bit of discomfort, then stop. The goal is to build a routine and let your body adapt to the mild stress without causing pain or excessive soreness.
Pain should never be your guide. If you feel any pain at all during or after a workout, it’s a sign you’ve done too much. Take a week off. Adjust your routine immediately by reducing weight, reps, or frequency. The aim is zero pain and only minimal muscle soreness. Proper form is paramount, especially for exercises targeting small muscles. Learning from certified trainers or reliable resources ensures movements are executed safely. Variety in training prevents overuse by alternating movements—switching from pronated to supinated grips, for instance, distributes load across forearm muscles. Rest and recovery, with at least 48 hours between sessions for the same muscle group, are essential, particularly for small muscles that heal slower.
I’ve been doing arm curls for years, working on my biceps. Then I learned about brachialis curls. The brachialis is a small muscle that has the potential to become quite a bit bigger and enlarge your forearms. I was so excited about building this muscle that I overdid it, and now six months later I still have nagging pain in both elbows. It’s easy to overdo something if you want quick results. Resist the temptation! Ultimately, results are the only thing that matter, but an injury is a result you don’t want.
Especially for former athletes: give yourself a year to build a platform, then gradually start working out hard enough to feel sore afterward.

Optimizing Recovery and Gains
Beyond the physical aspects of training, optimizing recovery is key to achieving fitness goals without injury. Adequate sleep is crucial for muscle recovery and growth. During sleep, the body releases growth hormone, which aids in tissue repair. According to an article in the Journal of Strength and Conditioning Research, sleep deprivation can negatively impact muscle recovery and performance.
Getting enough protein every day helps in rebuilding muscle fibers. You don’t need to get a huge dose of protein right after a workout — just keep up your protein intake throughout the day. Most people should aim for one gram of protein for every pound of lean bodyweight every day. That’s a lot. Break it into four times per day when you’re getting 30-50 grams. The best protein comes from animal sources, though vegetarians can compensate by getting even more. There is almost no upper bound on the amount of protein that supports muscle growth!
On the other hand, stress and fatigue can hinder recovery. Chronic stress elevates cortisol levels, which can break down muscle tissue and impair recovery. Managing stress through techniques like meditation or yoga can help maintain hormonal balance. Fatigue, whether from lack of sleep or overtraining, increases the risk of injury due to poor form and reduced coordination.
Body weight vs weighted exercise
There are so many good body-weight exercises that you can leave the weights out of your routine most of the time. Check YouTube for body-weight, floor, and movement exercises that are very challenging. Don’t think of yourself as a bodybuilder doing traditional movements. Lifts like deadlifts and overhead press are unnatural movements you’ll never use in real life. Work on doing compound movements that give you overall stability. Strengthen your back muscles without torturing them.
Instead of weighted squats, begin with bodyweight squats. Use a 30-degree wedge at the beginning to build good form. Get on a low platform and do toe and heel touches. Situps, pullups, and pushups are great starter exercises, and you can cheat them to get started — use bands, inclines, and isometrics like wall sits to build your foundation. Better yet, watch Lee Weiland take you on a smooth-movement journey and mix all your moves into fluid flow. Take small steps, ensuring that each step is taken with care.
Don’t be a specialist
As Peter Attia says in his book Outlive, you should choose about 20 different activities and become strong in all of them. It does not pay to be a pickleball or bench-press specialist. You want to work on big muscles, small muscles, balance, agility, stability, hand-eye coordination, carrying loads, off-center moves, lateral moves, floor moves, grip strength, rebound, jumping, core, even neck muscles. The body has a lot of muscles, so you can always be working something. Even when sitting or watching TV, you can do tibialis (toe) raises and push your hands together firmly, to flex your hand tendons. In the gym, you can do a lot of light activities from neck exercises to shoulder to core, movement, mobility, balance, hopping, step-ups, etc. So even if it’s just body weight at first, you can actually spend 90 minutes in the gym doing many different things and keep mixing it up all week with new movements. Do a lot of small things in the gym, but stop when your form starts to deteriorate because you’re too tired overall.
Mix cardio and resistance. You need both. Don’t do cardio on one day and weights the next. When you mix them, you can do more in a week than you can by separating them by day. An ideal routine would be a cardio exercise in the morning and a light workout in the gym in the afternoon. Every day.

Starting Slow and Building a Routine
Getting into a routine is crucial for long-term success. Start with 2-3 workouts per week. Focus on consistency rather than intensity. This approach helps your body adapt to the mild stress of exercise, reducing the risk of injury. Former athletes, in particular, need to be cautious. Their past experience might tempt them to push too hard, but age-related changes mean they can’t perform as they did in their youth. It’s essential for them to limit their weight and volume to about half of what their ego might suggest. For instance, if they feel they can lift 20 pounds for 10 reps, they should start with 10 pounds for 6 reps, then go do something else before getting fatigued. It may seem like too little, but you live to lift another day.
A 24-Month Progression Framework
The journey from beginner to intermediate should span 24 months, not weeks, to build resilience without risk. Think in terms of a 0-100 scale, where 100 represents maximum potential — competitive bodybuilder or powerlifter in your age category. Older adults should aim to reach approximately ten percent of their potential after one year, then 20-30 percent after two years. If you keep it up, after four years you’ll be close to 50 percent of your potential, which would be a transformation everyone will notice and will keep you strong and healthy for many more years. For those in their 70s and 80s, adjust that target downward to account for age-related declines in muscle mass, bone density, and flexibility. Imperceptible gains are better than quick wins. You should be frustrated with your lack of progress after three months and pleasantly pleased after nine months.
Some women worry they will become too big and look strange with all that muscle. This is a cartoon that won’t happen. To add five pounds of muscle would take two years of work for most women, and it would look natural and strong, not freakish. For most people, 10-15 pounds of muscle would be a good four-year goal, and it will make you look and feel fantastic.
The Long View
Slow and steady wins this race. Don’t be the person who says “I did something stupid and paid the price.” Preventing gym injuries requires patience and discipline. By warming up, progressing gradually, maintaining form, varying exercises, listening to the body, ensuring rest, and seeking professional advice, clients can safely navigate their fitness journey. Slow and steady wins the race, especially when the stakes are as high as maintaining mobility and independence in later life, ensuring a lifetime of active, injury-free living. Just wait until you get to year three!
Listen to Peter Attia talk with Kyler Brown, a sports-rehab specialist, about preventing injuries.
Rachel Rubin’s crusade to help women

At eight thirty each morning Dr Rachel Rubin arrives at her Bethesda clinic. A fresh stack of charts waits on her desk. Most describe women in their late forties to mid-sixties who feel tired, restless at night, and unsure why their own bodies seem unfamiliar. Only six percent of American women over fifty receive hormone therapy, mostly because of misunderstandings, bad reporting, and an undeserved reputation for causing cancer. Rubin calls that avoidable harm and has built her practice to close the gap. She tries to help as many women as possible, but there are more than she can handle.
In the entire United States, only about 1,300 clinicians have earned formal Menopause Society certification, a tiny fraction of the roughly fifty thousand obstetrician-gynecologists and nearly half a million primary-care doctors who could, in theory, prescribe hormone therapy. Against that limited pool stand more than sixty million women already past age fifty, plus another twenty-three million now entering the transition, the vast majority of whom could benefit from properly managed estrogen, progesterone, and (for some) testosterone. Yet fewer than one in twenty office visits by mid-life women results in a hormone prescription, a gap that forces many patients to drive hours or even fly across state lines to find competent care.
The three core hormones
Estrogen: This hormone steadies body temperature, supports memory, keeps skin elastic, maintains flexible artery walls, and is a critical component of building muscle and bone. Rubin prefers a skin patch or clear gel because those forms avoid the small clot risk linked to older tablets.
Progesterone: It protects the uterine lining whenever estrogen is present and, when taken at bedtime, improves deep sleep. Rubin starts with a micronized capsule if a woman still has a uterus. A progesterone-releasing IUD steps in when capsules cause daytime grogginess or mood change.
Testosterone: In women, testosterone is far less prevalent than in men, but it's also about 100 times more prevalent than estrogen. Testosterone allows exercise to increase muscle and bone mass, supports motivation, and restores sexual interest. Rubin prescribes a metered cream measured in tenths of a milliliter. Doses stay low and levels are reviewed until symptoms improve without skin or mood side-effects.
Strategy by life stage
Perimenopause: Cycles continue but hormone levels swing. Rubin eases symptoms with a low estrogen patch. She adds a small progesterone pill only when heavy periods or poor sleep persist. Testosterone is rarely used during this stage.
Menopause: Twelve months have passed without a period and estrogen production has dropped sharply. Most patients move to a moderate patch for joint comfort, mood stability, and bone support. Progesterone becomes mandatory for women with a uterus, delivered nightly or through an IUD. A daily micro-dose of testosterone joins the plan for muscle maintenance and libido.
Post-menopause: Needs depend on bone scans, lipid panels, and day-to-day function. Estrogen stays in place for bone and cardiovascular support, sometimes at a lower dose than before. Progesterone continues when a uterus is present and may be kept for sleep even after hysterectomy. Testosterone is trimmed or raised in small steps as weight, exercise, or skin response changes.
Patient stories
Carla, 57, improved sleep and mood on a standard estrogen patch plus a quarter millilitre of testosterone cream. Four months later chin acne appeared and impatience grew. Blood work showed testosterone high and estrogen low. Rubin halved the cream, increased the patch, and limited testosterone use to three days a week. Acne cleared and temperament steadied within six weeks.
Sandra, 52, reached menopause with disturbed sleep as her only complaint. A one-hundred-milligram progesterone capsule deepened her sleep but left her slow at breakfast. Dropping to fifty milligrams caused spotting. Rubin replaced the capsule with a progesterone IUD and restored the original estrogen patch. Sleep and daytime alertness both improved.
Ellen, 60, arrived with a testosterone pellet implanted by a wellness spa. Her gym results were strong, but hair thinned and mood swings were constant. Pellets cannot be adjusted after insertion. Rubin added a low estrogen patch and nightly progesterone, waited six months for the pellet level to fall, then switched Ellen to a measured cream. Hair loss slowed and mood stabilised while muscle strength held steady.
Carrie, 54, thought she couldn't take estrogen because she had had a blood clot in her 40s. Rachel explained that today's patches and creams are extremely safe and don't cause blood clots.
Patty, 73, said she couldn't have estrogen because she had breast cancer. Rachel told her she has many cancer survivors on estrogen patches and this was just another myth promoted by social media.
Maria, 63, seems to be playing a high-stakes game of hormone roulette. High estrogen eases her joints but triggers headaches. Lower estrogen calms her head yet stiffens her knees. Progesterone deepens sleep but slows recall. Testosterone brightens focus one month and feels emotionally flat the next. Rubin reviews the data every quarter and alters doses in small steps. The goal is the best balance available at the moment, not perfection.
Laurie, 74, kept having urinary-tract infections. Rubin explains that if women would use a cheap tube of vaginal estrogen cream every night, the US would save up to $22 billion just in treating urinary-tract infections alone, and save hundreds of lives. She even brought the cream to her own mother in the ICU and had to educate the doctors on why they should let her apply it.
Recently, Katie, 67, found me and asked if I would train her to build bone in the gym. The first question I asked was "How much estrogen do you have?" She looked up her number and said it was 12. I said "How are you going to build muscle and bone with no estrogen?" She agreed to go meet with Rachel and get started, because she doesn't want to break a hip when she's 80.
Persistent bleeding, fibroids, or a thick uterine lining can block safe estrogen use. For some women, no amount of progesterone seems right. In those cases, Rubin will recommend hysterectomy to reduce cancer risk.
Proven benefits
Balanced hormone therapy started within ten years of the last period lowers hot-flash frequency, slows bone loss, reduces hip-fracture risk, improves cholesterol balance, supports muscle maintenance when paired with resistance exercise, and improves sexual function. Early studies also suggest benefits for coronary health and cognition.
Rubin schedules forty-minute reviews because hormones seldom resolve in ten. Lab numbers and patient diaries guide each change. Two-thirds of women settle into a steady routine within a year. The rest need ongoing fine-tuning as their bodies adapt to the new reality.
Rachel Rubin wants every primary-care visit for a woman over forty to include clear explanations of hormone options, risks, and gains. Most new patients arrive believing they must tolerate their symptoms. Rubin prefers they leave knowing the tools exist, they are safe when used correctly, and adjustments will continue until daily life feels right again. She wants women to spread the word – hormone therapy saves lives, relationships, and provides a higher quality of life after menopause. She hopes young people will want to go to med school and help fill the need for more doctors to help more women. Listen to this entire conversation with Peter Attia, you’ll be glad you did …
I’m told that after this interview, her office received over 2,000 calls from people wanting to make appointments from all over the US. Now I know why she doesn’t answer my email requests to meet with her!
Should you take statins?

If you’re over 40 and your LDL cholesterol is above 100 mg/dL, it’s time to talk with your cardiologist about statins. High LDL signals a higher risk of heart disease, a major cause of death as we age. Statins, medications that lower cholesterol, are one of the most effective ways to reduce this risk. Despite online criticism, including from a few cardiologists, the evidence for statins is strong. This article explains the case for statins while addressing concerns and alternatives.
Rather than focusing only on LDL or VLDL, a better measure of heart disease risk is apolipoprotein B (ApoB). This protein carries harmful cholesterol through your blood, contributing to plaque buildup in arteries, and it’s easy to measure directly. It should be less than 90, and lower is better.
Statins are an important tool in lowering ApoB — which you want to get as low as possible. A low dose of statins can give you most of the benefit with probably no side effects. For example, after I had a stroke, my doctor raised my prescription to 40 mg Atorvastatin, which is standard after a stroke. After about a year, I asked to go back down to 20 and he said sure, that would be fine, so I did. Ask your doctor about starting with the smallest dose he/she recommends.
In my view, statins are just a part of your journey to better heart health. You can lower ApoB more by reducing insulin resistance and inflammation than you can by taking statins. If you’re really serious about controlling ApoB, your A1c should dictate what you eat. If your A1c is 6.0 or greater, you should eat no carbs and be in ketosis. If you can get it down under 5.7, then you can add carbs in, but carefully. And you can do exercise — especially hard exercise — to keep your arteries soft and reduce plaque. Managing stress matters too. All these things combine to help reduce your risk of heart disease. On top of all those things, statins can reduce your risk of cardiovascular disease even further.
Online, you’ll find plenty of anti-statin arguments, sometimes from cardiologists, warning about muscle pain, liver problems, or claiming cholesterol isn’t the main issue. These points deserve consideration—side effects like muscle pain are real for a small group. But large-scale meta-studies, the most reliable form of medical evidence, consistently show that statins significantly cut heart attack and stroke risk for most people over 40 with high ApoB or other risk factors.
The meta-studies
Meta-studies look at many large-scale trials, throw out those that are poorly designed or underpowered, and try to summarize the total evidence found across the good ones, which are usually randomized, placebo-controlled (RCT). Metastudies must be taken seriously and can’t be ignored. They offer the strongest evidence on statins’ role in reducing cardiovascular risk. Below is a compact summary of major findings, focusing on adults over 40 with risk factors like high apolipoprotein B (ApoB).
Cholesterol Treatment Trialists’ Collaboration (2010, 2015)
Scope: 26 RCTs, >170,000 participants, primary and secondary prevention.
Findings: Statins cut major cardiovascular events (heart attacks, strokes, deaths) by 20-25% per 1 mmol/L LDL reduction. Benefits consistent for those over 40, with or without prior heart disease. Low-dose statins effective, side effects rare (<1% myopathy).
Cochrane Review (2013)
Scope: 18 RCTs, >56,000 participants, primary prevention.
Findings: Statins reduced all-cause mortality by 14% and cardiovascular events by 25% in people over 40 with risk factors. Side effects minimal.
Baigent et al. (2016)
Scope: 28 RCTs, >180,000 participants, broader populations.
Findings: Statins lowered heart attack and stroke risk by 24% per 1 mmol/L LDL drop, effective across ages and risk levels. Benefits outweigh risks (e.g., slight diabetes increase in 0.1%).
No major meta-study concludes that statins should generally not be used by the general population over 40 with cardiovascular risk factors, such as high apolipoprotein B (ApoB) or LDL cholesterol above 130 mg/dL. The most comprehensive meta-analyses, like those from the Cholesterol Treatment Trialists’ Collaboration (CTT, 2010, 2015) and the Cochrane Review (2013), consistently show statins reduce cardiovascular events (heart attacks, strokes) and mortality by 20-25% per 1 mmol/L LDL reduction in adults over 40, with benefits outweighing risks for most, even at low doses. People who argue against statin use cite smaller studies with less statistical power, and they often offer “remedies” with almost no high-quality studies behind them. Statins lengthen lives for those who tolerate them.
Other factors
One aspect of heart disease is genetic. Some people have the LP(a) gene, which predisposes them to having high cholesterol and heart disease. These people should be doing everything they can to lower cholesterol, with the general approach being statins, diet, and exercise.
For the roughly 5% of people who can’t tolerate statins due to side effects like muscle aches, there are alternatives. Medications like colesevelam, ezetimibe, red-rice yeast, or PCSK9 inhibitors (expensive) can also lower ApoB or reduce cardiovascular risk through other mechanisms, such as decreasing inflammation. Your doctor can design a treatment plan tailored to your needs.
Are statins overprescribed?
It’s probably true that some people who are taking statins shouldn’t be, while many others who should be taking statins aren’t. Guidelines are continuously monitored and were updated in 2024 to indicate that more low-risk people probably shouldn’t be taking them. A good up-to-date cardiologist would be better at making this decision than all your Facebook friends put together.
Summary
If your LDL is high, you should take action to improve your health. Statins, especially at low doses, are backed by decades of research showing they extend life. Combine them with lifestyle changes, and you’re building a strong foundation. Don’t let online debates steer you off course. Get your ApoB tested, have an honest conversation with your cardiologist, and find the plan that’s right for you. Use your brain, not your heart, to decide what’s best for your heart.
If you’re over 50, there’s much more on this website for you to learn about health and longevity. A good place to go next would be my facts page, or if you’re interested in supplements, check out my stack page. You should also see my store.
Finally, here’s Dr Peter Attia talking about statins …
The Luxury Retirement Community of the Future
Here’s the message: don’t underestimate old people, they can do amazing things and will be healthier and live longer when they are working hard doing things they enjoy and find meaningful.

Yuichiro Miura, standing on top of Everest at 80 years old.
I give webinars and talks to people over 60, because I want to help them live longer. I also talk with people who run retirement communities, because I want to help their residents live longer. I look at a lot of websites of retirement communities. They all have some things in common: images of people drinking alcohol, dining, and engaging in leisurely fun. They show some yoga, shuffleboard, and “fitness” classes. What they don’t show is people getting stronger and more independent.
It’s not their fault. It’s just the way it’s always been done. It’s what the market wants. Actually, it’s what the market thinks they want. People who run retirement communities are focused on providing activities and keeping residents busy. But that is solving the wrong problem.
Antifragile, a term coined by Nassim Taleb,describes systems that gain from disorder, to distinguish them from things that are merely robust or resilient. Fragile things break under stress and robust things survive it unchanged, while antifragile things improve when stressed. The human body is antifragile: muscles grow stronger with resistance training, bones grow with stress, and the immune system strengthens through exposure to pathogens. Startups often thrive in volatile markets by adapting to shocks quickly. Evolution itself is antifragile—random mutations and environmental stressors lead to stronger species over time.
I talk about the top-seven things likely to kill you (Cancer, diabetes, heart disease, neurodegeneration, falls, etc.), but the more I look at those websites, the more I think these people are all dying from the same thing:
Boredom
It’s good they have community, because loneliness will shorten your life. It’s good people are busy, because it’s better than not busy. But it seems to me that people over 65 or 70, no matter where they live, are missing a sense of purpose and wanting to make a difference. The weeks are structured, the weeks are busy, but they all blend together. Classes and activities come and go. Holidays come and go. People celebrate by eating more. There is no hustle. Zero hustle. People read books, magazines, watch Netflix, have coffee with friends, and they wait for the next activity on the schedule.
Retirement communities are like full-time cruise ships. They have everything you need to develop full-blown diabetes and require assistance using the bathroom.
But humans are built to hustle. They thrive on it.
This is not limited to retirement communities, it’s a national public health emergency.
Handle with care
Recall the statistics: a measurable increase in deaths occurs on or around birthdays. In the U.S., a study of 25 million deaths showed a 6.7% increase in mortality on birthdays, with men aged 20–29 seeing a 25.4% spike. In Switzerland, birthday deaths rose by 13.8%, especially among those over 60. French data from 2004 to 2023 showed a 6% average increase, peaking at 24% for men aged 18–40 and 29% for centenarians. People can prevent themselves from dying if they have something to look forward to.
And yet most people seem content to play a bit of bridge and pickleball, do some yoga, pretend to be exercising in the swimming pool, and show up for some activities. Judging from the websites, they spend most of their time drinking alcohol with friends and meals. And 73 percent of US adults are either overweight or obese. And people in senior residences are as overweight and obese as the rest of the population.
If you have seen the movie Wall-E, you know where this is heading.
We die from disuse and atrophy — not from “saving our energy.” We die from lack of purpose, overcoming obstacles, and commitment — not “activities.” Older people are treated too gently. They are coddled and accommodated. If you have read The Comfort Crisis, you’ve seen many examples.

People are overmedicated. People taking drugs for hypertension, osteoporosis, diabetes, or overweight are making themselves sicker. This is true for many other areas as well. They could just exercise and eat better. Furthermore, 95 percent of women over 50 are not on hormone-replacement therapy, which promotes osteoporosis, prevents building muscle, and shortens their lives.
And the current “longevity” fad is lots of fancy tests, scans, treatments, and drugs. Without exercise. Because exercise has low profit margins.
Please handle roughly
I remember once I was in Macedonia or Azerbaijan, I forget, but I ran into some older Americans who were there as election monitors. They didn’t have a lot of money. They worked with an organization that places them into a country for a few months before and during an election. I’ve met some amazingly talented woodworkers still in the shop creating at age 70. I know an 80-year-old author writing his 26th book. I know an 80-year-old ski instructor in Japan who skis 60 days a year. The world record for an 80-year-old running the 100m dash is 17 seconds (I can do 20). About 500 athletes over 80 compete every two years in the National Senior Games. The oldest man to climb Everest was 80 and the oldest woman was 73. The oldest woman to climb Mt Kilimanjaro was 89. I could go on and on.
They didn’t accomplish these things by taking it easy. They did it by putting their boots on day after day and working hard.
The future of retirement?
With that in mind, I want to re-imagine retirement communities for Gen-X. I’m assuming this is for high net-worth people who can afford it, though I think many of these ideas will trickle down. I’m also assuming this is for independent living more than assisted living, although I think assisted-living people are in far too much comfort and don’t have to struggle enough, which causes them to deteriorate further. I’m just putting ideas out here with the goal of stimulating conversations among people planning to build new communities or upgrade their existing facilities.
The goal is to make it so residents:
learn new skills.
have to struggle and stay at it.
have to work together to do new things.
have to rely on each other as team members.
discover a sense of purpose and accomplishment.
can measure and track progress and celebrate their wins.
have big things to look forward to.
have a full schedule of things to look forward to, so there’s always the next challenge.
People need projects. Think about that. What projects do they do in a retirement community? Their week is filled with “activities,” but no projects. It gets routine. Projects have schedules, mini-deadlines, sprints, reviews, you have to buy stuff and bring it in and coordinate. You need to develop skills and improvise when things go wrong. Then there’s the sense of accomplishment after it’s over. Why are retirement communities so quiet? Why aren’t they bustling hubs of people working on things and waiting impatiently for the Amazon truck to arrive and making videos and uploading them to the YouTube channel and sharing it with everyone they know?
People need outside stimulation. I visited my mom at her assisted-living facility in Denver. She had lunch with the same three women every single day. I sat down with them, opened my laptop, asked one of the “girls” her childhood address, and showed her her old neighborhood on Google maps. She was entranced. She saw the homes of her neighbors, and memories came flooding in — people and things she hadn’t thought about in decades. She marveled at the new shopping center and the changes to the local park. Soon, I had a line of people saying “Do me next!”
People need responsibility. You know what they don’t have? Responsibility. No one’s counting on them. No one’s waiting for them. No one needs them to do something. This might be fine for many people, but it’s counter to our nature. People like to work. They like to have something that needs to be done. They like to have the satisfaction that comes when they serve others. Why can’t the residents be responsible for cooking dinner for the entire facility — including the staff — once a week? That would put some responsibility on some shoulders, and they would quickly form groups and systems to do it creatively. I once lived on a kibbutz in Israel with about 1,000 residents and cooked American-style pancakes for everyone one Sunday morning — plenty of people pitched in to help.
People need connection. Why aren’t seniors connected across the globe? There are already hundreds of online communities. Could those be boosted? Could there be annual awards and recognition? Could there be useful networks to help solve real-world problems? Could they help coordinate disaster relief or expeditions? Could they purchase time on telescopes and explore the cosmos? People from retirement communities should be able to find each other, collaborate, and create new things together without needing any “adult supervision” from staff. Some of the things I propose don’t have enough people in any one community to get lift. But across many communities, “birds of a feather” can find each other and start collaborating.
People need purpose. Even rich people who go on luxury around-the-world cruises eventually get tired of it. People feel better when they are doing something they feel is meaningful to others. This drive helps them live longer and stay in better shape for the future.
Family activities with goals. Most family visits are calm, sit-down, food-oriented visits where grandchildren are forced to give up their screens and game time to pretend to be interested in what’s going on with grandparents and to report on school, friends, life, etc. It’s more like a board meeting and not something to look forward to. What if the kids were there to work on setting a new world record or building a Rube Goldberg machine to make a YouTube video? What if they were shooting a movie or designing a new game? What if they were doing experiments with big magnets? What if they were using AI to solve a problem someone had at the community? What if they came to work with grandparents on making gifts for their friends or a project for school or needed some modifications to their skateboard?
Dealing with restrictions and limitatations. Of course, old people can have all kinds of restrictions. But some are false. Hypertension, insulin resistance, osteoporosis, even aching knees and bursitis can all be reversed with diet and exercise. Cancer survivors can get ridiculously strong — one cancer survivor now guides other cancer survivors to the top of Mt Kilimanjaro regularly! Wherever you are, you can improve — a lot. Probably a lot more than you think.
If you believe what I propose here is dangerous and people can get hurt, keep in mind that probably the most dangerous thing you can do is sitting around, reading, playing games, drinking alcohol, and gaining weight.
Here are some suggestions.
Health and fitness
Insulin resistance: Insulin resistance is the foundation for heart disease, cancer, Alzheimer’s, and many other problems. All people at every age should be aware of their A1c number and reduce it to under 5.7. This should be the first priority for any residence program. I see too many websites featuring a “plant-forward menu,” and that’s exactly what people who are insulin resistant should not be eating. These dietary models are based on outdated low-fat diet fads that played a strong role in creating the obesity epidemic.
In the retirement community of the future, residents should commit to becoming insulin sensitive and get the support they need to do that. They should not go on medical programs for weight loss, like Semaglutide — medical interventions like that should be for people who want to go to the old-style rest homes where people get fat and die young.
Gym: most “gyms” in retirement communities are toys. If you want to see a real gym for people in their 60s and 70s, look at Greysteel. It’s a very different place, where old people are doing extreme things safely. In fact, I have a complete business plan for what this gym would look like and how it would be different from other gyms, and it would attract members from the entire community, not just residents. And the residents can run it! You don’t need staff except for cleaning and a few other things the residents don’t want to do. What about bodybuilding competitions? Don’t underestimate old people.
“Stronger a year from now than you are today” — which retirement community offers this? None. Yet that’s exactly what they should be about. The older you get, the more you should work to build and maintain muscle and bone. The gym experience should be hard. Old people are capable of handling a lot more weight and stress in the gym than you think. The goal for every senior should not be to become superman or woman but to be stronger a year from now than they are today. No matter who they are, that yearly goal adds to independence and creates many years of quality life. I have a program for doing this safely.

This is Steve Taylor. He’s 69. Don’t underestimate old people.
Weight loss: If retirement communities know how to get residents to lose weight, they are holding back their secrets. I’d be surprised if very much actual weight loss is going on. I’m willing to bet that the average person gains weight over the years at these facilities.
We know a lot about weight loss now, and my view is that most “registered and licensed” dieticians don’t know any of it. Their textbooks are full of 30-year-old, low-fat dogma. It’s not their job to force anyone to lose weight, but it should be their job to give people the option of enrolling in a weight-loss program that actually causes people to lose weight. The proof of their competency is in the numbers — how good are they at helping motivated people lose weight and keep it off?
We need better programs. Most people are insulin resistant, and those people should be in ketosis. The harder you work out, the better your cardiovascular system gets, but too many facilities are gentle and don’t push residents. If they want the results, they must be willing to put in the work. No sugar. No alcohol. No cheating. It takes a good strategy for each person, structure, hormones, and many hours in the gym, but they will be very happy when they see the results. This is true for most people at any age. Everyone has pre-existing conditions, but most people can get far better results than they are getting now.
Research teams: People should not rely solely on their doctors for advice. Too often, they resort to Facebook groups or Google searches. But some people know how to do scientific research, literature reviews, and look at data. And there are many good experts publishing on many topics.
Residents could take some initiative and put together teams to help figure out how to solve medical problems. They probably wouldn’t be much worse than the doctors they’re seeing now. Why wait around for “experts” to tell them what’s best? At the very least, they should be well educated. They don’t have to be doctors, but they can help put things in perspective and get a second opinion from another doctor. They can learn how statistics are used and misused in medicine and science in general. A good example is osteoporosis medicines, which no one should be on. If your doctor prescribes Fosamax or Boniva, you should find another doctor. Research groups can help make better educated guesses than many doctors do, and ask pertinent questions. Sure, they may need a guide, but ChatGPT is a pretty good one.
Indoor activities with purpose
Activities should require very minimal staff, because most communities have residents who are capable and can be trained to be the staff. Being a staff member is another purposeful job that gets you out of bed and serving others, plus they often have to move heavy equipment around, which helps keep them strong.
Most of these can be run as clubs, where people pay a membership fee and get a locker. Can be open to the public as well. Don’t underestimate what the residents can do — more and more will be fully digital and online. There will be fewer and fewer AOL email addresses.
Woodshop: most people think a woodshop is a noisy, dangerous place with lots of high-speed spinning blades and common injuries. This is not the case. Today’s woodshops are very carefully ventilated with full dust collection, the machines have lots of safety guards, and woodworkers make sleds and carriers to keep their cuts straight and their fingers away from the action. Injuries are now quite rare. Don’t underestimate old people — they are capable of running, using, and maintaining a wood shop with all kinds of machines. And it lets them produce things they are proud of and give to their families or make for their community. Need cutting boards or serving platters? Want a ping pong table, a foosball table, a lamp, or a chess board? A puzzle or a sculpture? Don’t order one. Build one.
Metalshop: Same as above, but there’s more computer-driven equipment.
3D printing: Supplies are fairly cheap. There’s always something new to learn.
Performance space: I’m sure there are some retirement communities where people volunteer, participate, and create exciting cultural events, where the residents are the performers and entertainers. This should be the norm, but it takes residents to volunteer and build up a great program and produce great performances. I’m sure some of the better ones also involve groups in the community. There’s huge potential here.
Ping pong: Sounds silly, but ping pong at a high level really challenges hand-eye coordination. All retirement communities should not just have ping-pong tables but elevate the level of ping pong playing to tournament and master’s level. It’s fast. It requires quick reactions. There’s no reason some of the best and most competitive master’s ping-pong players in your city shouldn’t be coming from retirement communities. Looking forward to tournaments and having high-level opponents will help preserve motor units and neurons.
Volleyball: Same thing with volleyball, but the normal ball is a bit heavy and can damage hands and wrists. So play the same game with a much lighter, foam ball. Let’s set a standard for a new kind of ball, keep everything the same, and make this new sport very competitive. Compete against other retirement communities. Have regional championships. This is far better than “activities” for seniors.
Pickleball: The problem with pickleball is it’s too easy. I know at the pro level that’s not true, but at the local level it is. Doubles is far too easy. If you do pickleball, make it singles, and get everyone to play at a high, competitive level. Again, tournaments against other communities will encourage residents to upskill and enjoy meeting other pickleball enthusiasts and enjoy sharing a good protein shake after a hard match.
Juggling: Anyone can get into juggling, and the sky is the limit. There are thousands of levels, tons of videos, and teams can compete against each other online. There are camps and competitions around the world. Juggling is one of the best ways to preserve motor skills and coordination.
Climbing wall: People think climbing walls are dangerous, but they aren’t. A well designed and run climbing wall is a fantastic way for people in their 70s and even 80s to develop muscle and fitness. This is functional muscle. It combines balance, coordination, and movement. It improves grip strength and builds skills people can be proud of. People pair up and support each other. And it will draw grandchildren in to spend time with their grandparents.
Magic camp: Anyone can learn magic tricks. Good magicians can put together an act and go around town performing. They can perform at hospitals, schools, community centers, and festivals. You have to practice, learn, watch videos, get coaching, be determined to master each trick. Grandchildren will show up for lessons.
Learning lab: learn a new language together. Study physics or chemistry. Focus on one particular time in history, like the Diet of Wurms or how the pyramids were built, and make a video explaining it. Learn what causes strokes. Take the free video classes at MIT and Stanford. Learn to speed read. Compete in brain games. Do it as a group project and help each other. Have meetings. Divide up the work. Set deadlines. Deliver deliverables. Teach others.
VR: Using VR, people can go on all kinds of adventures. Have you tried exploring the space station or climbing a mountain? You can visit places around the world and interact with others. Why not have a network of people in retirement communities all having online adventures and events together? You can even play team games and put on performances.
Lego lab: Lego enthusiasts have come up with the Great Ball Contraption contests. They are held all over the world. They design mechanisms for moving balls along a conveyor line, and they are wild. See 2012, 2016, 2022. Do you think a lego lab might attract a few grandchildren to come visit?
Run a store: In Washington DC, there’s a “Made in DC” store, where everything is locally made. Why not have a store that the seniors can run all by themselves? It doesn’t have to be on campus, it can be in town, pay rent, pay for staff and services, and break even as a nonprofit. Residents can do the books, buy products, run checkout, do marketing, events, and more. Or run an online store and use the profits to support good causes. Strange as it may sound, people will stay alive longer simply because others are counting on them to do their job.
Make products: Seniors can make everything from chocolates to guitars to t-shirts to cutting boards to iPhone cases and much more. They could set up a small factory, make products, sell them online, do marketing, PR, and much more. Why not? A successful factory can hire local teens or others and help grow the economy.
Host a TEDx event: Anyone can host a TEDx event. Get people from all the retirement communities in your city together and host one. Let them organize, prepare their talks, build the signs, run the event, and share the results with their families afterward.
Digital crafts: People can collaborate to design all kinds of things using online design tools. They can build 3D models, scenes, animations, simulations, games, apps, and use AI to create films. By working online, they can have mentors and collaborators around the world. Seniors should be able to come up with a good idea for an app or a website, launch it, and use the network of seniors connected online to promote it.
Publishing: People can write books, make videos, create online classes, share their photography, hold webinars, and much more. This could be done at scale, so someone who’s giving a lecture on the Bernoulli effect could find a wide audience of interested people around the world. No one at his local community is interested, but by connecting communities, new markets open up. You can even set up a letterpress print shop and make all the cards, signs, menus, booklets, and everything else everyone needs. They could write and record music. They could create a science channel and make videos. They could print things their grandchildren want, so they work with them on projects. Doing it by hand the old-fashioned way is fun, creative, and satisfying. Don’t underestimate old people!
Contests: Every month there are contests for all kinds of things: paper-airplane design and flight, puzzle boxes, origami, one-off bicycles, egg drops and catapults, houses of cards, domino falls, Geoguesser, building musical instruments from scrap, yoyo competitions, bodybuilding, and much more. Plan. Train. Compete. Win or lose doesn’t matter.
Outdoor activities with purpose
Don’t underestimate old people. The worst thing they can do is go on a cruise. On a cruise ship, everyone is overweight, everyone eats, lays down, and sleeps. Then there’s a bit of entertainment or losing money in the casino. This is not what today’s retirees want or deserve. They need to get moving.
Many seniors enjoy gardening, but they don’t work very hard at it. The average farmer is healthier and lives longer than the average person in a retirement community. Residents can grow food for their community. They can put in the long hours and hard work to raise vegetables, fruits, herbs, and other things that will benefit the people who live there. And take pride in what they have grown. This sounds like work for the staff, but it’s actually great for the residents. They can even set up a farmer’s market or go participate in one.
Want a bowling alley? Build one. Want a pickleball court? Learn to build one. Need a cart to carry things around? Build one. Weld up the frame and assemble the parts, then paint it and admire your handiwork. These kinds of things are so much more satisfying to do if you built it yourself and maintain it. No staff needed — building the thing is every bit as good an activity as using it, so who cares how long it takes? Forget the crossword puzzles and card games — build things.
Rucking is so beneficial for older people that it should be a standard activity. Rucking is walking and hiking carrying extra weight on your back. Everyone should be rucking 2-3 times a week. It helps build hip and spine bones and muscles. It’s far better than walking. Walking doesn’t help people lose weight or gain muscle and bone. Every community should have a rucking club. Why can’t seniors walk a few miles, get all their gardening supplies or groceries, put them into their backpacks, and walk back? Sound too difficult? Those people will outlive the others who don’t.
Hiking keeps you agile. Hiking with weight on your back keeps you stable and strong. Those who hike twice a week will be far stronger than those who don’t.
There are so many other opportunities. Community members can be referees at soccer games, umpires at baseball games, and otherwise contribute to children’s sports in the community. You think they wouldn’t jump at the chance? Don’t underestimate old people.
Transportation is definitely an issue. We don’t want most people over 80 driving cars. But there are so many other options now, I believe each community will find good ways to get their seniors where they need to go. As long as people want to do things in groups, the costs are usually reasonable.

This is Flo Meiler at age 84. She has over 700 medals in track and field.
Travel activities with purpose
I would like to create travel experiences that are the opposite of cruises. One proposal I have is to take grandparents and their grandchildren to East Africa, to climb Mt Kilimanjaro and then go on safari. Why climb the mountain first? Because it’s hard. To climb to the top of Africa, you need to spend a year getting ready. If you’re bringing your grandchildren on safari, then you need to spend that year with your grandchildren hiking, walking, rucking, preparing, learning about the route, minimizing risks, and — voila! — doing a project together with them. Because the prize is three weeks in Africa, a lot of kids will give up screen and game time to prepare with grandma and grandpa. And guess who’s going to carry most of the luggage?
There are big events every year where people get together to do very hard challenges and obstacle courses. Examples: Grit, Tough Mudder, Red Bull 400, Spartan race. Why don’t we create a series of events for seniors? They can train, prepare, pack, and go compete against people from around the country, similar to the National Senior Games. If you think this isn’t going to exist, you are underestimating old people.
Wouldn’t it be great to set up a senior travel agency to plan these kinds of trips around the world? It could be a virtual company with everyone working online. Guess who could work there?
These are just a few ideas showing how market trends may develop and how senior living may adapt. I’d like to see a senior living facility that pushes people and doesn’t underestimate them. It’s not for everyone, but it would attract its own clientele, and they would probably live to be far healthier and far longer than most people in most retirement communities.
To learn more about longevity and antifragility, explore this website and contact me with any questions.
The Continuous Glucose Monitor Fad will Fade

When Tom, a 55-year-old executive and beach-tennis enthusiast, got his annual blood work, he was rattled. He saw an A1c of 5.8%. Having just read a book on increasing healthspan, he thought: “That’s prediabetes,” imagining insulin shots and diet overhauls. Eager to take charge, he jumped on the wellness bandwagon, went to Amazon and bought a $100 continuous glucose monitor (plus extra supplies) to track his blood sugar in real time. He figured spikes after meals would show if his insulin was faltering, and he could watch his progress on an app. But weeks of fixating on the app left him confused. What was he really measuring, and what did it really mean?
How A1c works and doesn’t work
A1c measures the percentage of hemoglobin coated with glucose, reflecting average blood sugar over two to three months. A reading of 5.7–6.4% suggests prediabetes; below 5.7% is normal, and 6.5% or higher indicates diabetes. It’s a snapshot, not a real-time insulin gauge. But A1c can be misleading. High readings can result from anemia (e.g., iron deficiency prolongs red blood cell life, increasing glucose attachment), kidney disease, or ethnicity—African Americans and Hispanics often have higher A1c without elevated glucose. Low readings can stem from blood loss, sickle cell disease, or frequent blood donations, which shorten red blood-cell lifespan. Some people have smaller blood cells (e.g., in thalassemia trait) or higher red blood cell turnover (in certain genetic variants), both within normal ranges, but these distort A1c by altering hemoglobin exposure to glucose. For Tom, mild anemia likely nudged his 5.8% higher, not insulin resistance. And it could have been temporary.
The CGM fad
Tom’s pivot to a CGM reflects a biohacking craze, but these devices, built for diabetics, mislead non-diabetics. CGMs track interstitial glucose, showing post-meal spikes (e.g., 160 mg/dL from pasta) or stability (under 130 mg/dL). Big spikes might hint at insulin resistance, but normal glucose can hit 140–180 mg/dL after carbs, affected by stress or sleep. A week of data can’t diagnose insulin resistance, which is a slow-burn condition. Tom’s pizza spikes were normal.
Obsessing over CGM numbers, fueled by YouTube influencers, risks pointless diet tweaks or anxiety. Even Peter Attia, a guy I respect a lot, wears one. Why? He keeps saying he’s not a fan of overtesting. But he probably gets more podcast views when he shows people his glucose levels on his phone app. Peter is smart enough to debunk the fad and spread the message that they are only useful for people who are injecting insulin.
Peter gives one scenario where a CGM can benefit a non-diabetic patient: if a person is wearing a monitor for months and you have a glucose profile, then when giving a new drug or changing something, you could see if that has any effect on insulin resistance if the glucose numbers increase, and then if you reverse the change and the numbers go back down to baseline, you can assume it was whatever you changed. That’s kind of a billionaire biohacker toy, because if you’re measuring A1c every six months or so, that will generally tell you things are going in the wrong direction. But to have people wearing monitors just to get a baseline and then watch for changes seems over the top to me. Maybe it can help patients that were diabetic and are now under control, but I don’t think it’s practical to measure every little thing on normal people.
The OGTT solution
If Tom wanted to know about insulin resistance, which doesn’t change very quickly, he should’ve chosen the gold standard — an oral glucose tolerance test (OGTT). After a 75g glucose drink, blood glucose is measured at fasting, 1-hour, and 2-hour intervals. A 2-hour reading below 130 mg/dL is normal; 130–190 mg/dL flags prediabetes. At $50–$200, often paid by insurance, it beats CGMs ($50–$100/month) and provides better data. Dr. Rachel Rubin cautions, “Misinterpreting normal responses with trendy tools like CGMs can lead to unnecessary interventions.” Not only that, because other factors can influence glucose numbers, Tom has no idea what his actual insulin-resistance level is.
Remarkably, Tom later read this blog and went to get an OGTT. It showed a 2-hour glucose of 125 mg/dL. Is that normal? To put this in context, I’ll put both ranges into a table to help you interpret the results:
Tom’s value of 125 mg/dL is more accurate than his previous A1c number, so he should use that. It’s a good number, but it helps to understand what he should do and not do at this point.
Most people talk about the “glycemic index” of a particular food (candy bars are higher than crackers), what really matters is the glycemic load. Tom should be aware that eating a small chocolate-chip cookie is different from eating two small cookies. People in his range should not worry about eating carbs, but they should try to limit how much sugar they get at one time. More glucose spikes will tend to raise his insulin resistance. A glucose monitor would show this, but common sense says it’s better not to put the second cookie in his mouth.
Now that Tom knows he’s in the normal range, he doesn’t need another test unless he feels he’s been getting too much glucose. He can keep playing beach tennis, live a normal life, and not worry too much about measuring biomarkers. In general, a blood test once a year should show you anything to worry about and investigate. Symptoms will tell you even more.
Skip the fad. Don’t over test. Get your A1c measured every six months and adjust your lifestyle to bring that number down to 5.5 or lower. If you don’t get a reliable number from an A1c test, get an OGTT. But the goal is not to measure. The goal is to change behavior.
To learn more, read my Facts page.
Disclaimer: Consult a healthcare provider before pursuing medical tests.
To learn more, read my Facts page.
Disclaimer: Consult a healthcare provider before pursuing medical tests.
The little-known benefits of vaginal hormone delivery

As I have mentioned, hormone-replacement therapy transforms lives for women from their 40s to their 80s, giving women the ability to build bone and muscle, prevent cancer, and many more benefits. Here, I’ll talk about the benefits of local hormones applied as vaginal creams and rings. Not only do most women not know about these products, but if you’re reading this and you’re a woman, you can probably benefit.
Vaginal creams reduce menopause-related challenges like vaginal dryness, painful intimacy, reduced sexual desire, and life-threatening urinary tract infections (UTIs). Using DHEA (dehydroepiandrosterone), estradiol, or compounded creams, these treatments deliver profound benefits—safe, affordable (thanks to Mark Cuban’s Cost Plus Drugs pharmacy), and life-changing.
A Lifeline Across Decades
In their 40s and 50s, women in perimenopause often face vaginal dryness, discomfort, and reduced sexual desire, even on systemic HRT. Jessica, a 48-year-old teacher, struggled with these issues and recurrent UTIs. A compounded estradiol-testosterone cream from Cost Plus Drugs, costing $15 monthly, eliminated her symptoms in weeks. “No UTIs, and my sex life is vibrant again,” she says, thriving at home and work. DHEA (Intrarosa, 6.5 mg daily) converts locally into estrogens and androgens, boosting lubrication by 115%, reducing pain during intercourse by 108%, and increasing desire, arousal, pleasure, and orgasm by up to 49%, per studies. Estradiol (Vagifem, applied 2–3 times weekly) strengthens vaginal walls. Compounded creams, blending DHEA, estradiol, progesterone, or testosterone, offer tailored relief, with progesterone reducing inflammation and testosterone enhancing libido—crucial for perimenopausal women seeking sexual vitality.
In the 60s and 70s, these therapies restore comfort. Linda, 68, used a $18 DHEA-progesterone cream to end UTIs and painful intimacy. “I’m enjoying romance again,” she says. UTI prevention is critical, as menopause thins vaginal and urinary tissues, increasing infection risk that can escalate to sepsis. Studies show vaginal hormones cut UTI rates by 50%. Marjorie, an 83-year-old ICU patient post-heart surgery, avoided a deadly UTI with daily DHEA cream. “It kept Mom safe,” her daughter said.
At 79, Sarah struggled with vaginal dryness, urinary urgency, and a UTI about once a year. A DHEA-testosterone cream relieved her discomfort, improved bladder control, and restored her confidence. “I used to get a UTI yearly, but I haven’t had one since starting the cream,” she says. “I’m back to enjoying book club and lunches with friends without worry.”
Vaginal Rings: Simple and Effective
Vaginal rings, like Estring, are flexible, silicone devices inserted into the vagina to release low-dose estradiol for 90 days. Women insert them (like a tampon) and replace quarterly, with no daily upkeep. Studies show 80–90% improvement in dryness, discomfort, sexual function (including desire and orgasm), and UTI prevention by supporting urinary tissues, ideal for busy or mobility-limited women.
The labeling problem
The FDA’s labeling for vaginal hormone products, like estradiol creams and rings, often includes warnings about risks like blood clotting, which apply to oral estrogen but not low-dose vaginal therapies. These outdated warnings, rooted in systemic oral-estrogen risks (oral estrogen is no longer used), create confusion, giving doctors, pharmacists, and nurses pause. Many hesitate to prescribe or administer these treatments, unsure of their safety due to mislabeling, which limits patient access to life-changing care. Dr. Rachel Rubin, a urologist, has advocated for change, stating, “The boxed warnings on vaginal estrogen are outdated and misleading; these products are safe with minimal systemic absorption, yet the FDA clings to systemic hormone risks, limiting access to life-changing care” (2023 interview with The Washington Post). Her efforts underscore that vaginal hormones, with negligible systemic effects, don’t carry the same dangers, yet mislabeling persists, hindering proper prescribing and use.
Safe, Affordable, and Impactful
These therapies are safe across decades, with localized action avoiding risks like blood clotting. Trials report only mild side effects like discharge. Mark Cuban’s Cost Plus Drugs offers estradiol cream for $13.21 versus $293.66 through Medicare. Cuban told PBS in 2022, “Our approach at Cost Plus Drugs… show you our actual cost, mark it up 15%, add $3 pharmacy handling fee and $5 shipping… has really had an impact.” Dr. Rachel Rubin, a urologist, states, “Vaginal hormones prevent UTIs by more than half, improve arousal, orgasm, and lubrication, and could save the healthcare system $6 to $22 billion annually by reducing infections and doctor visits.” A tube of vaginal cream used to cost hundreds of dollars, now it’s only $18 plus shipping.
You may not have even heard of this, which shows how misinformation travels. Doctors should be talking with all their patients about adding local delivery of hormones to any woman’s health regime. All women should explore vaginal hormone therapy for its ability to enhance sexual desire, arousal, pleasure, orgasm, protection, and overall quality of life, while preventing costly infections—whether in perimenopause, living vibrantly in her 70s, or in the ICU in her 80s. Consult your healthcare provider to explore FDA-approved Intrarosa, vaginal rings, or compounded creams through Cost Plus Drugs or local pharmacies.
Disclaimer: Consult a healthcare provider before starting treatment.
Explore my website and blog to learn more about women’s and men’s health over 50.
Hormone replacement therapy for women

I talk with a lot of women over 50, and I’m surprised that the vast majority have never tried Hormone Replacement Therapy (HRT). When I ask “Why?” they shrug their shoulders and say it’s just not for them. But they don’t know that. They don’t know the difference it could make. They have been led to believe that by the persistent myth that estrogen causes breast cancer. As you’re about to learn, hormone replacement therapy prevents cancer and supports healthy aging.
History of HRT
In the 1960s, HRT emerged to ease menopausal symptoms, with estrogen widely embraced by the 1990s for hot flashes and bone health. The 2002 Women’s Health Initiative (WHI) study wrongly alarmed millions by overstating risks of estrogen-progestin HRT, like breast cancer and heart disease, causing a major setback for women’s health research and trust in hormone therapy. Part of that was caused by oral estrogen pills, but most of the problem was in bad data.
Although it was front-page news, later analysis of that same data debunked WHI’s flaws, and more studies continued to show HRT is safe and effective for most when started early with modern methods like creams or patches. Today, personalized HRT is a cornerstone of menopause care, with doctors tailoring doses and delivery to individual needs, underscoring the importance of early action. Still, today fewer than 6 percent of women are on HRT - one of the greatest public health failures of the last 100 years. If you want to live better for longer, talk with your urologist or endocrinologist about trying HRT.
HRT for Women in Perimenopause
Perimenopause, often in your 40s, brings irregular periods, hot flashes, and mood swings. Estrogen creams or patches can stabilize symptoms and improve sleep. There are also rings and vaginal creams. If you have a uterus, add progesterone (micronized pills or creams) to protect against endometrial issues. There is no single solution: some women feel calmer, others bloated, others irritable. In most cases, it’s best to start with estrogen first and set a good level before adding progesterone.
Stay ahead—experiment with low-dose HRT early. Hysterectomy patients can use estrogen alone. Discuss delivery methods with your doctor to find what works, adjusting for side effects. Delaying worsens discomfort, so start now to stay comfortable.
Women in Their 50s
Menopause in your 50s often intensifies hot flashes, vaginal dryness, and fatigue, disrupting daily life. Estrogen creams or patches (avoid oral pills) can reduce symptoms by 80% and boost mood. To prevent endometrial cancer, almost all women with a uterus should be on progesterone (micronized pills, rings, or creams). With enough experimentation, you should find a delivery method that works for you.
During menopause, symptoms and conditions can change. It would not be unusual to change your dose and delivery method at least once during this period. Stay ahead of it. Try options early, like patches for steady delivery, and pair with exercise. Some women like to inject themselves, they say it gives them much more control. Don’t settle for brain fog or fatigue. Get your HRT and get into the gym. Acting promptly keeps you vibrant.
Women in Their 60s
In your 60s, 40% of women face hot flashes, and vaginal dryness or urinary issues increase. Vaginal estrogen creams or inserts are low-risk and effective. Systemic estrogen (creams or patches) or progesterone (micronized pills or creams) can aid energy, but heart risks grow. Progesterone’s effects differ—some feel great, others sluggish.
Don’t let symptoms linger—try vaginal estrogen and a progesterone ring early. Explore safe delivery methods with your doctor, and consider non-hormonal options if systemic HRT isn’t suitable. Regular check-ups ensure safety.
Women in Their 70s
Hot flashes (10–15%) and vaginal dryness (over 50%) persist in your 70s, affecting comfort. Vaginal estrogen creams or inserts are safe and effective. Systemic estrogen or progesterone (micronized pills or creams) is riskier due to heart and dementia concerns but may help severe symptoms. Progesterone can be calming or disruptive.
Act early—experiment with low-dose vaginal estrogen. Hysterectomy patients can use estrogen alone. Discuss delivery options with your doctor, and add strength training. Starting now preserves quality of life.
Women in Their 80s
In your 80s, vaginal dryness or urinary issues can reduce comfort. Vaginal estrogen creams or inserts are safe, improving intimacy and reducing UTIs. Systemic HRT is rarely started due to heart and dementia risks, but continuing prior HRT may work. Progesterone responses vary—some benefit, others don’t.
Stay proactive—try vaginal estrogen early. Explore delivery options with your doctor, and maintain check-ups. Starting an exercise program alongside HRT supports muscle growth and independence.
Yes, there is some risk of starting late. But there are risks to not starting. Talk with your doctor to see if HRT is right for you. If your doctor doesn’t mention the benefits, get another doctor.
Benefits of HRT:
Symptom Relief: Reduces hot flashes (up to 80%), night sweats, vaginal dryness (50–60% prevalence), and mood swings, improving sleep and quality of life.
Bone Health: Lowers osteoporosis risk (50%) and fracture risk by 24–34%.
Heart Health: Supports cardiovascular health if started early, potentially reducing heart disease risk.
Comfort and Mobility: Enhances energy, muscle strength, and urinary health, reducing UTIs and fall risks.
Individualized Care: Tailored options (creams, patches, inserts, micronized progesterone) suit varied responses, especially for hysterectomy patients needing only estrogen.
Risks of Not Using HRT:
Persistent Symptoms: 40% of women in their 60s and 10–15% in their 70s endure hot flashes; 50–60% face vaginal dryness, leading to discomfort and UTIs.
Bone Loss: 50% osteoporosis risk, with 20% bone loss in 5–7 years, increasing fracture risk (20–30% hip fracture mortality).
Mood and Energy Decline: 2–3x higher depression risk, plus fatigue, brain fog, and reduced vitality.
Missed Opportunities: risks like heart disease and dementia rise with age.
Testosterone for Women
Testosterone, often overlooked in HRT, can be a powerful addition for women at any age, addressing low libido (40–50% prevalence post-menopause), fatigue, and muscle loss (3–5% per decade). Low-dose testosterone creams or gels can boost sex drive, energy, and mood, while supporting muscle strength to reduce fall risks. It’s off-label, so work closely with your doctor to try it early, monitor for side effects like hair growth, and pair with estrogen for balanced benefits. Don’t wait—exploring testosterone can enhance vitality and confidence, especially if symptoms persist.
Summary
If you want strong muscles and bones and you don’t want cancer, it’s time to stop imagining that HRT is not for you. See your doctor to explore HRT — at the very least, estrogen. Experiment with delivery methods to find your fit—HRT can enhance your life at any stage.
If you’re still not convinced, listen to this conversation between Dr Peter Attia and Dr Rachel Rubin. If you want an online hormone doctor, see Pema Bioidentical. I have no affiliation with either. Here’s a roundup of online providers.
Learn more about my longevity coaching service by exploring this site. You may want to start on the facts page.
Everything your doctor doesn’t know and won’t tell you about osteoporosis
CAVEAT: Before starting any supplement, drug, or exercise program, talk to your doctor. Understand that the risks of inactivity are probably higher than the risks of exercise. I’m not your doctor. You assume any risks from taking or not taking the advice here.
If you're over 40, your peak bone density and mass are in the rear-view mirror. As we age, we all lose bone mass, unless we can manage to build it back up. Osteoporosis, which affects over 10 million Americans over 50, can lead to fractures that steal independence. According to Dr Doug Lucas:
50 percent of adults over 50 are at risk of a fracture.
50 percent of women and 25 percent of men will suffer a fracture from poor bone quality in their lifetime (I’ve had 10).
Women have a higher chance of a fragility fracture than they do of heart attack, stroke, and breast cancer combined!
24 percent of people over 60 with a hip fracture die within 12 months.
Independence is permanently lost for 50 percent of patients who fracture a hip.
I broke both hips in my early 50s. My bones are now far stronger than they were 20 years ago. I have learned how to build bone, and you can too.
In this article, I lay out what I think is the useful information about osteoporosis for most people. I make the case against drugs and for specific bone-building exercise, and I go through all the useful supplements. Then, I show a video on what does work — resistance and impact exercise, plus balance and stability exercises, supported by the right diet and supplements. You can do it, it’s not difficult, and it doesn’t take much time. If you don’t want to read about the drug issues, just skip to the exercise section at the end, it’s the most important.
This article should take you about 40 minutes to read and watch, and it should save many people at least one fracture later in life.
If you're interested in supplements, you'll find specific recommendations on my stack page. If you’re interested in a consultation, see my pricing page.
I have a special note about the AlgaeCal company at the very end.
What are bones?
If you're over 50, you should have an interest in maintaining bone density and mass, which means you should be planning to grow bone, because you are almost certainly light on bone in your hips and spine right now. That's why I recommend this book, The Osteoporosis Breakthrough, by Dr Doug Lucas, who explains everything more precisely but with more words than I can dedicate here. It’s actually a short, very readable book.

Bones are living tissues that constantly remodel, balancing the activity of cells that build bone (osteoblasts) and those that break it down (osteoclasts). Calcium provides rigidity, collagen provides flexibility. Together, they create a composite material stronger than either alone, like reinforced concrete (collagen as rebar, calcium as cement).
The human skeleton contains two primary bone types: cortical (compact) bone and trabecular (spongy) bone, each with distinct roles and traits.
Cortical bone, forming 80% of skeletal mass, is dense and strong, creating the hard outer layer of bones like the femur. It provides structural support and resists bending.
Trabecular bone, found inside bone ends (e.g., in vertebrae), is porous and lattice-like, making up 20% of bone mass. It supports marrow, aids shock absorption, and remodels faster (10–20% annually vs. cortical’s 2–5%).
Plus, your bones function as red-blood-cell factories to boot!
Approximately 10–20% of your skeleton is remodeled annually in adults, and your entire skeleton turns over in 7-10 years. Isn’t that amazing?
The process of building bone relies on nutrients like calcium, vitamin D, vitamin K, and collagen, which form the bone’s mineral and flexible matrix. However, the key driver of bone growth is mechanical stress—carrying weight and absorbing impacts. Soccer players have thicker, stronger bone in their lower kicking leg by about 20 percent. Tennis players have stronger bone in their hitting arm by 30-40 percent. Ancient tribal skeletons of our past relatives who paddled boats had huge shoulder capsules and arm bones from paddling, while people living in mountainous regions have stronger, thicker knees and ankles. The majority of people in wheelchairs for over five years have moderate to severe demineralization in their hips and spines, and more than 80 percent of people in wheelchairs after ten years have osteoporosis, regardless of age. Without stress, bones weaken, no matter how many supplements you take.
And bone mass disappears for women as soon as they start to lose estrogen from menopause:

The above graph is misleading. You think it represents everyone and that bone demineralization is natural, but that’s wrong. What that graph actually shows is that we become less active as we age. People who continue to do hard exercise, lift weights, or participate in certain sports do not have the same amount of demineralization as everyone else. Bone density is a function of a) having the right ingredients (calcium, estrogen, some other minerals) and stimulus (impact, heavy loading, and stress).
Look at people in their 80s: look at their wrists. They are tiny. Why? No stress! If you want to keep it, you have to use it.
The bad news: running, tennis, cycling, swimming, even hiking and most other sports don't build your hips and spine. Yoga, pilates, and walking are about the same. Almost everyone over 40 is demineralized, and the hips, spines, and wrists are often the weakest links. No, you are not the exception, and no, mountain biking does not do it. If you row competitively, you probably are one of the few people with a strong spine and hips.
The key concept is that your body builds enough bone to meet the needs of your anticipated activities and no more. This is called Wolff’s law. Spend a year building up your legs with exercise and your body will happily build the bone needed to support that activity. Stop and your body will begin dismantling that bone within days. That's why demineralization is such a risk for astronauts, who train with big rubber bands daily in space, and why it's so dangerous for them to walk when they get back after a few months in a zero-gravity environment.
Now I’m going to cover supplements, drugs, diagnostics, estrogen, diet, and then exercise, fall prevention, vibration plates, and maintenance at the end.
Supplements
Calcium
Calcium is the main mineral in bone and the main supplement doctors prescribe. Studies, like a 2007 analysis in The Lancet, show that 500–1200 mg of calcium daily can slow bone loss in postmenopausal women by about 1% per year. Vitamin D, often paired with calcium, helps your body absorb it, reducing fracture risk in those with low levels. But here’s the catch: while calcium and vitamin D prevent further loss, they don’t significantly build new bone without exercise. If your DEXA scan shows a slight uptick after starting calcium, it’s likely because you’re losing less bone, not growing more.
The best kind of calcium to get is the calcium found in leafy green vegetables. That's why I recommend AlgaeCal Plus, which is made from algae, so it's essentially the same as getting your calcium directly from vegetables. AlgaeCal Plus gives you 360 IU of calcium in the morning and 360 IU at night, for a total of 720 IU of bioavailable calcium.
Do you need more than 720 IU of calcium? The answer is … we don’t know. Recommendations for vitamin D range from 800 to 40,000 IU per day! But it’s not how many units you take, it’s how much vitamin D is in your blood. So you need to test and adjust, and it’s probably different in summer vs winter. Peter Attia recommends 60-80 ng/mL. Others recommend around 30-40 ng/mL. The amount you need to take to achieve this depends very much on you and your lifestyle and where you live. On the other hand, Dr Brad Stanfield says we should be careful and that most recent studies show that there are dangers to getting too much vitamin D (but it takes years to do the damage, so don’t worry).
The Endocrine Society recently lowered their recommendations to 600 IU daily for people 50-70 and 800 IU daily for those over 70. Clearly, we need more and better research.
The way I think of it now is that it makes sense to get the basic 800 IU that comes with AlgaeCal Plus and then supplement to hit a blood-level target. Some people are naturally low and need more. Some people get a lot of vitamin D from their diet, while others don’t. If you’re outside all summer, you may want a supplement during winter, or you may have enough from the 800 IU in AlgaeCal Plus. To do it right, you need a blood test in about January. Generally, if you’re not deficient in vitamin D, you probably don’t need to supplement very much. But the jury is still out.
Magnesium
Magnesium has so many benefits, and the negative effects of not enough magnesium are so bad that most athletes and bodybuilders now take magnesium. But it also plays a critical role in bone building. It stimulates the activity of osteoblasts and enzymes from the phosphatase group, which are involved in the bone formation process. Most good calcium supplements, like AlgaeCal Plus, come with magnesium.
There are actually eight kinds of magnesium. Optimal to support muscle growth are magnesium citrate and glycenate or bisglycenate. The recommended daily allowances (RDA) for magnesium are:
400-420 mg. per day for men 19-51 years of age
310-320 mg. per day for women 19-51 years of age
350-360 mg. per day for pregnant women
Adults over 51 should aim for the upper limit of the recommended range for their gender
Split doses (e.g., morning and evening) to improve absorption. You could take a citrate in the morning and then a glycinate at night, which aids sleep, enhancing recovery.
Calcium and heart disease?
Calcium supplements may contribute to arterial plaque buildup, potentially increasing heart disease risk, but the evidence is conflicting. A 2010 study in BMJ found that taking calcium supplements without vitamin D raised the risk of heart attack, possibly because high doses cause calcium to deposit in arteries. However, a 2016 study in the Journal of the American Heart Association showed no clear link between calcium supplements and artery calcification in women over several years. Dietary calcium from food seems safer than supplements, and risks may vary based on dose and vitamin D use.
More research is needed, but for now I believe the researchers who say taking the amount of calcium you get in your daily dose of AlgaeCal Plus is not a cardiovascular risk, as long as you’re also getting enough K2 (see below).
Kidney stones
Calcium supplements can help keep your bones strong, but they might also raise your risk of kidney stones, those razor-sharp little crystals that form in your kidneys. A study from the 1990s showed that eating calcium-rich foods cut kidney stone risk in half for men, because the calcium binds with oxalates and prevents them from reaching the kidneys. But a 2006 study found that taking 1000 mg of calcium supplements daily increased stone risk by about one-fifth in older women, especially if taken on an empty stomach.
The key is how you take supplements. Taking high doses of calcium without food or water can spike calcium levels in your urine, making stones more likely. To stay safe, stick to 400 mg or less per dose, take it with meals, and drink plenty of water—8 to 10 cups a day. Food sources are your best bet for calcium, but if you need supplements, talk to your doctor, especially if you’ve had kidney stones before.
Know your list of foods high in oxalates. When you eat these foods, be sure to take a calcium supplement at the same time, so they bind together in your stomach and don't go into your bloodstream. Otherwise, the oxalates can make their way to your kidneys and wait there for the calcium ions needed to build a stone.
Collagen
Collagen supplements are popular for skin, nails, hair, and joint health. Collagen is a peptide (a kind of protein complex) harvested from cow, chicken, and fish bones, and chicken eggs. Does collagen also help build bone? Collagen forms the flexible framework of bones, but evidence for bone benefits from supplements is thin. Collagen supplements probably help joints rebuild, and it can’t hurt for building bone. But if you skip the collagen and just take AlgaeCal Plus, you probably won’t be at a disadvantage. I tell my clients that if you have joint pain, or if it helps your hair and nails, take collagen.
It’s possible that taking collagen is helping you build some small amount of bone or making your bones more resilient. You’d never be able to see the difference on a DEXA scan, or even a REMS scan. If you’re a big strong person who’s lifting heavy, you can take it or leave it. But if you’re on the skinny side or getting more frail, it can’t hurt to get your daily collagen. I take mine every day, because I do notice a difference in my joints.
Vitamin D
Vitamin D is like a key that unlocks your body’s ability to build strong bones. It helps your gut absorb calcium and ensures calcium gets deposited into your skeleton to form hard, healthy bone tissue. Without enough vitamin D, even a calcium-rich diet won’t fully protect your bones, leading to weak bones or conditions like osteoporosis.
But more isn’t always better. Recent research, like a 2023 study in JAMA Network Open, warns that taking too much vitamin D (over 4000 IU daily) can cause problems, such as high blood calcium levels, which may harm your heart, kidneys, or even weaken bones. To stay safe, aim for 800–2000 IU daily from food (like salmon or fortified milk), sunlight, or supplements, and check with your doctor before taking higher doses. If your blood test shows you are deficient, take enough to get into the higher range of normal, but make sure you aren't getting too much. Get a reasonable amount of vitamin D and get outside more. Keep in mind that people in their 80s and 90s need extra vitamin D, simply because their skin is less efficient at making it.
Vitamin K2
Vitamin K2 is like a traffic cop for calcium, guiding it to your bones to keep them strong and away from places it shouldn’t go, like your arteries. It activates proteins, such as osteocalcin, that help calcium stick to the bone matrix, making bones denser and less prone to fractures. A 2013 study found that K2 supplements (180 mcg/day of MK-7) slightly improved bone density in postmenopausal women after three years, especially when combined with calcium and vitamin D.
You can get K2 from foods like natto (fermented soybeans), egg yolks, and cheese, but many people don’t eat enough of these. Supplements can help, but they’re not a magic fix—K2 works best with exercise, which signals bones to grow, and nutrients like calcium and vitamin D. Taking too much K2 (over 200 mcg/day) is rarely harmful but may not add extra benefits. K2 is in most calcium supplements these days, you don't need extra.
Strontium: a red herring
Strontium, another supplement closely related to calcium in the periodic table but denser, raises the most questions. Found in products like strontium citrate, it mimics calcium and can lodge in bones. Clinical trials, such as a 2004 study in the New England Journal of Medicine, showed strontium ranelate increased DEXA scores by 1–3% over three years and cut fracture risk by 20–30%. Sounds promising, right? But strontium’s heavier atomic structure absorbs more X-rays, making bones appear denser on DEXA scans than they truly are. Up to 75% of the density gain may be a DEXA artifact, not stronger bones. Plus, strontium can cause blood clots you don't want.
Doug Lucas says that he sometimes recommends strontium for some of his patients, it’s probably not necessary, it can potentially support bone growth, but we still don’t have good studies that isolate the effect of strontium vs other micronutrients. I’m not sure when he recommends it, but he says less than half of his patients want to take it, and he’s “open to that.” It’s not his default recommendation. I wonder whether patients taking strontium are just crowding out their calcium and if calcium would do as good a job or better. Since I’m not your doctor, this is something to discuss with your endocrinologist.
Boron: a non-key ingredient
Boron plays a supportive role in bone formation by enhancing calcium, magnesium, and vitamin D metabolism, modulating hormones like estrogen, and potentially stabilizing the collagen matrix. Its effects are modest, with 1–3 mg/day from diet or supplements improving nutrient retention and BMD slightly, especially in postmenopausal women or vitamin D-deficient individuals. However, boron cannot replace calcium’s mineral role, collagen’s structural role, or exercise’s critical stimulus for bone growth. It’s a helpful but non-essential player in bone health. You probably get enough boron in your normal diet anyway.
Osteoporosis drugs
Now we come to the elephant in the room: the big-money osteoporosis drugs that don't work.
Bisphosphonates: a trap for getting your money and making your bones worse
Bisphosphonates like Fosamax (alendronate), Boniva (ibandronate), and Actonel (risedronate) are billion-dollar drugs marketed for osteoporosis, promising to reduce fracture risk "by 50 percent." But the benefits are actually an accounting trick.
Drugmakers boast a 40-50% relative risk reduction in fractures. Impressive? Not when you ask about the absolute risk. For women with osteoporosis, the annual hip fracture risk is 1-2%. A 50% relative drop means the risk of fracture went from 2.2 percent to 1.1 percent. That’s an absolute risk of 1.1%. Over five years, treating 100-200 women prevents one fracture. Meanwhile, there are serious side effect risks: 1 in 1,000 face osteonecrosis of the jaw, a painful, disfiguring condition, and 1-5 per 10,000 suffer atypical femur fractures—see the image below. Esophageal irritation, heartburn, and rare heart rhythm issues add to the toll.
But the drug companies make sure the story is told to search engines the "right" way. All large language models produce the same result when asked about the risks of bisphosphenates:

This is exactly the story drug companies want told. They manipulate the journal summaries and abstracts to achieve what I call online narrative supremacy. Most doctors believe these drugs actually help, because most doctors don’t know the difference between relative and absolute risk.
Bisphosphonates don’t build bone; they trap old, brittle bone, reducing bone quality. “Drug holidays” are recommended after 3-5 years to reduce risks, yet long-term safety remains unclear. Worse – these drugs realign the structure of your bones to make them brittle and fragile, resulting in “atypical fractures” where your bone breaks like a stick of chalk …

An atypical fracture caused by drugs: this is not how bones naturally break.
Not to mention the life-threatening jaw problems. Osteonecrosis of the jaw is a condition where areas of the jawbone become exposed and do not heal properly, leading to bone death. Symptoms may include jaw pain, swelling, gum infections, loose teeth, or exposed bone. Patients are advised to not have any extensive dental work done while on these drugs.
If your doctor recommends bisphosphenates, don't ask questions and don’t argue. Walk out. Find a better doctor.
New horizons in osteoporosis treatment: the post-bisphosphonate era
Are there other options? Yes, there are. Bisphosphonates have long had the lion’s share of the marketing budget (and profits), pretending to reduce fracture risk by slowing bone breakdown. However, for patients who can’t tolerate them, experience fractures despite treatment, or face long-term risks like osteonecrosis of the jaw (ONJ), or have to take their required drug holidays, newer post-bisphosphonate therapies offer hope.
At least, they offer hope to drug companies seeking more profits. Because — tada! — the new drugs solve the problems created by the old drugs!
Or … do they?
Prolia (Denosumab), a twice-yearly injectable monoclonal antibody, reduces relative vertebral fracture risk by 68%, with an absolute risk of ~4.8% (from 7.2% to 2.4% over 36 months). Ideal for bisphosphonate-intolerant patients, but stopping it triggers rapid bone loss and a 3–5% absolute risk of rebound fractures within 6–14 months. ONJ and atypical fractures occur in less than1% of patients, with infections in the range of 4% (absolute risk). Okay, so only 4 out of 100 people get infections.
Forteo (Teriparatide), a synthetic parathyroid hormone, increases bone density by 6–9% and reduces relative vertebral fracture risk by 65%, with an absolute risk of about 10% (from 14.3% to 4.6% over 21 months). That’s a significant reduction in fractures. Forteo only costs $41,100 yearly, and the daily injections only cause nausea or hypercalcemia in about 10% of patients. ONJ risk is ~0.02%, and osteosarcoma, seen in animal studies, has not yet been seen in humans.
Evenity (Romosozumab), a monthly sclerostin inhibitor, boosts bone density by 15% and cuts relative vertebral fracture risk by 73%, with an absolute risk of about 3.7% over 12 months. That is statistically significant. However, a 30% relative increase in heart attack risk (absolute risk: ~1–2% higher vs. placebo) limits its use in those with cardiovascular history, and its $21,900 annual cost would give you a completely setup home gym in just 12 months.
With billions in annual sales, these drugs enrich Big Pharma while offering marginal benefits compared to exercise and nutrition, which strengthen bones safely, give you more ability to prevent falls, and make you feel great. It is possible that some people with severe risk of fracture could benefit from these drugs, but if you’re reading this, you’re almost certainly not one of them.
All about DEXA scans
A DEXA scan is the most common — but not the best — way to measure bone density. In my view, too many people get DEXA scans. They are mostly a marketing tool to get people moving on the conveyor belt to taking drugs they shouldn’t be taking in the first place.
After you get a DEXA scan, you get a T-score, which is your bone density compared to that of an average 35-year-old. If you’re 50 or 60, of course your score is going to be negative! Why would they compare you to people 20 years younger? Because then they can give you the diagnosis of “osteopenia,” which labels you “at risk of a fracture,” and just a few years later, they can say you finally have osteoporosis, it’s time to start your lifelong drug regime (minus the holidays).
Think about bone-density tests for a minute. The only time you need to test anything in medicine is if you’re planning to do something different depending on the outcome of the test. You’re looking at two paths of action, and the test tells you which one.
Scenario A: You just got a DEXA scan and learned that your bones are not as strong as they could be. What do you do? You keep taking your supplements and you get into the gym and build bone! You wake up every morning and say “It’s another day to build bone, and I’m going to do it.”
Scenario B: You just got a DEXA scan and learned that your bones are as strong as they could be. You’re above average. What do you do? You keep taking your supplements and you get into the gym and build bone! You wake up every morning and say “It’s another day to build bone, and I’m going to do it, because if I’m not building bone I’m losing bone.” You don’t ease up. You don’t worry about building too much bone (that doesn’t happen).
In both scenarios, you’re going to do exactly the same thing after the test. So, why test?
Unless you have a very rare condition, you don’t ever need a bone-density test. If your doctor recommends a bone-density test, make sure he/she tells you the two different paths you will take based on the results, because it’s most likely to be taking a drug. Otherwise, forget the test and get your bones into the gym.
If NASA could prevent bone demineralization with a drug, they would, but they can’t. That’s why they have a resistance gym in the space station.
Estrogen: a key signaling factor
Estrogen, often thought of as a female hormone, plays a vital role in building and maintaining strong bones in both women and men. In women, estrogen helps bones grow by slowing down the activity of cells that break down bone, allowing bone-building cells to add more bone tissue. This is especially important during youth and pregnancy, but after menopause, when estrogen levels drop, bone loss speeds up, raising osteoporosis risk. A 2002 study in The Lancet showed that estrogen therapy in postmenopausal women can preserve bone density and reduce fracture risk.
In men, estrogen is less abundant but still critical. Men produce estrogen by converting testosterone, and it works similarly to protect bone by limiting bone breakdown. A 1998 New England Journal of Medicine study found that low estrogen levels in older men were linked to weaker bones and higher fracture rates.
Not all women can or should have hormone replacement therapy, but most can. If you can take it, you will build more bone, build more muscle, and feel better with more estrogen. If your estrogen is low, it doesn’t matter what you do in the gym, building muscle and bone will be very limited.
I recommend every woman talk with her doctor and, if she can, try HRT for at least six months. If you don't like it at that point, think twice about getting off, because you can't build as much bone without it as you can with it. As with any treatment, you need to understand the costs, benefits, side-effects, and tradeoffs.
If you’re looking for a good HRT doctor, I recommend Pema Bioidentical, Midi, and Winona.
Diet
You hear a lot of people recommending all kinds of diets to improve bone density. The research on which diet is optimal for preventing bone loss is generally poor and mixed. It seems clear that various diets have an impact, but there are many other confounding lifestyle factors that make it difficult to tease out. Most studies show that young people should consume dairy products to grow bone in their teens and 20s, some studies show that consuming dairy products, especially fermented-milk products like yoghurt, help prevent bone loss. Some research says that a plant-based diet is bad for bones, while others point out that plant-based milks are probably just as good.
Almost all researchers agree on two things: 1) get as much calcium you can from leafy green plants, and 2) you need enough protein to support healthy bones.
Protein
We don’t know that much about protein and bone building, but here’s how to think of it: you should get the optimal amount of protein for health and longevity. This will support you in building muscle and bone. While the protein doesn’t directly contribute to building bone, a low-protein diet will deprive you of bone density.
I have been vegan most of my life. At age 51, I fell and broke my right hip. At age 53, I fell and broke my left hip. This is my actual x-ray:

That’s a definitive diagnosis of osteoporosis. We now know that vegans break far more bones than non-vegans, vegans do not grow as tall as meat eaters, and that a low-protein diet is almost guaranteed to demineralize your skeleton.
In addition, insulin resistance probably contributes to osteoporosis. If you’re insulin resistant, reduce carbohydrates, and if you’re pre-diabetic or worse, eliminate them from your diet.
The general recommendation today is to consume one gram of protein per pound of ideal bodyweight per day, and meat protein is better protein. While I still don’t eat meat, I do consume a lot of whey protein and high-protein yoghurt, in addition to as much tofu, pea protein, protein bars, shakes, and nuts as I can get. I’m always trying to get as much protein as possible, which means on some days I probably meet my one-gram-per-pound goal.
People who consume a lot of meat don’t have that problem, but they should probably limit red meat to about 20 percent of protein calories to help prevent heart disease. Or maybe not. We really don’t know.
People in their 80s and 90s need even more protein. There’s even evidence that it helps people with Alzheimer’s function better. Keeping up your protein intake will support your bone-building program, while not getting enough protein will work against it.
Genetics and Osteoporosis
Osteoporosis is heavily influenced by genetics, similar to how genetics determines lung cancer risk — some people can smoke all their lives and be healthy and not die of cancer, but the choice to smoke increases the chances of getting cancer dramatically. Similarly, your genes account for 50–85% of bone mineral density (BMD) variation, setting your bone strength baseline by age 30. Genes like COL1A1 (collagen) or VDR (vitamin D) determine peak bone mass and loss rates. You do inherit much of your two parents’ genetic fracture risk. A parent’s hip fracture raises your risk of fracture at age 70 to 5–10 percent vs. around 1–2 per year for a person of the same age.
But even genetic “superstars” aren’t immune — poor diet, inactivity, or menopause can erode BMD by 10–20 percent. A sedentary lifestyle will still decrease bone mass in these people, while weight-bearing exercise and calcium/vitamin D intake can boost BMD by 2–5 percent, countering genetic risks. Protection is relative, not absolute. For example, research on LRP5 mutations shows carriers have stronger bones lifelong but can still face age-related decline if calcium intake or physical activity is inadequate. Genetic testing for key variants can pinpoint vulnerability, but understand that the older you get, the more bone you’ll lose, even if it’s at a lower rate than for other people. Regardless of your genes, the remedy is still the same … exercise.
The key to building bone: exercise
To build bone, you need the raw ingredients, but you need to give your bones the signal to build. And only exercise does that (see the section on the LIFTMOR trial, below). There are three general kinds of exercise that contribute to bone building and stability.
Resistance exercise must be very heavy. You need a lot of weight or heavy resistance bands to compress your bones enough to give them the signal to build. It’s not impossible, it’s just not what most people do. Research shows that bench pressing or squatting half your weight isn’t enough. You have to go more into powerlifter territory, lifting your own body weight and more. Or you need to do a lot of reps. That’s beyond most recreational gym goers. If you’re going to do it, it’s going to be with a barbell rather than with dumbbells or kettlebells. Certainly, more lifting is better, but it takes years of conditioning and skill building to compress the bones enough to get them to grow. If you can do it, you’ll be building muscle for longevity as well.
But most people can’t do that, and for us, there is impact exercise. I’d rather have you watch a video than describe it, so I made one. This is, as far as I can tell, the best, most thorough impact video on YouTube. Please set aside time to watch it:
Plyometrics are fast moves that develop explosive and reactive power. They help build bone, and they give you more ability to jump, hop, and get out of a tricky situation. A good example is hopping on one leg and trying for distance and accuracy, maintaining your balance once you stop. Hopping up to a step or platform in ever-increasing increments on one leg is fantastic. The more you practice, the more you’ll energize and retain small muscles that will help you avoid an accident.
Fall prevention
The other kind of exercise that contributes to bone health is exercise to help with stability, so you’re not a fall risk. You won’t break a bone if you don’t fall in the first place. There are a range of exercises that reduce your fall risk.
Balance training starts with balancing on one leg and going up from there. You should constantly be training for balance, which is why I never touch the handrails of any stairs. The other one is the toe squat, where you are resting your butt on your heels and your heels are off the ground. This is an easy thing for 20-year-olds to do and a difficult thing for 50-year-olds to do. I practice it about ten minutes every day. Finally, there’s the test of putting on your sock and then shoe and tying your shoe while balancing on the other foot. If you can keep doing that as you age, you’ll be less of a fall risk.
Stability training helps prevent falls. I work with all my clients on balance, hopping, squatting, and other movements to keep from losing stability. For example, walking backward up an inclined treadmill is one exercise that will improve the muscles at the back of the leg and prevent falls.
Step-ups and step-downs are important exercises to help you navigate terrain as you get older. I spend a lot of time on many types of step-ups and step-downs, so I’m always prepared to go down stairs, jump down, squat, get up off the floor with no hands, etc.
Carrying loads helps build and maintain bone. You can carry weights in the gym, you can carry a backpack. You can also get a weight vest and do walking and hiking under load. I would rather see you walk 3 miles carrying weight than 6 miles unweighted. See my list of weight vests and packs in the store on this site. See my video below on carrying your groceries home on your back.
Motor unit training involves quick, precise moves, like you would do in tennis, basketball, or ultimate frizbee. These are cutting, turning moves that involve acceleration and torque. Parcours, tire training, pylons, trail running are all good examples. Fast motor units are some of the first to go, which is why 40-year-olds aren’t as agile as 30-year-olds. You can train this, but it takes a good trainer or set of videos to show you what to do.
Preventing falls is as important as building bone to resist a break. All these exercises combine to give you stronger joints, stronger hips and spine, and stronger wrists and arms, so when you’re 80 you have the abilities you had in your mid-60s. Keep it up every day and you’ll be in far better shape than your peers as they decline.
Maintenance
As I mentioned, if you’re not building bone, you’re losing bone. Both happen slowly, but a year can make a significant difference. Once you’re on a bone-building program, you’re on it for life. You don’t get to take time off.
What does that mean, exactly?
When you travel, you should plan to exercise and get in your impact work. It’s not that difficult, you can do it in your hotel room. You should be squatting and lifting as much as you can, even if it’s just your own body weight (push-ups, squats, wall-sits, etc.)
Suppose you get sick and are unable to exercise. If it’s a week, focus on getting better and go back to your regular routine as soon as you can. But if it’s longer, you should try to find a way to do your impact work. If I were going to be laid up for more than a few weeks, the first thing I’d do is order a vibration plate and learn to use it properly. Take this seriously. At the very least, put some effort into not losing bone.
The LIFTMOR trial
The LIFTMOR trial (2015–2017), conducted in Australia, assessed high-intensity resistance and impact training (HiRIT) in 100 postmenopausal women with low bone mass (osteopenia or osteoporosis). Over 8 months, participants performed twice-weekly supervised HiRIT, including deadlifts, squats, overhead presses, and drop landings from a hang on a bar for impact. HiRIT significantly improved bone mineral density (lumbar spine: ~2.9%, femoral neck: ~2.2%), muscle strength, balance, and functional mobility compared to a low-intensity control group. Bone turnover markers showed reduced resorption. the Functional Reach Test showed enhanced stability. Only one minor musculoskeletal adverse event was reported, confirming HiRIT’s safety and efficacy for bone health.
This trial and others show that resistance and impact training have a huge effect on bone density, make you feel great, contribute to other health factors, and make you even more stable and less of a fall risk in the first place.
Vibration plates
You may have seen or tried a vibration plate. They look like this:
Studies of vibration plates show that they don’t tend to build bone, but they do help reduce the rate of loss of bone. The key is hips and spine. It’s not a silver bullet, it’s not the only thing you should rely on to build bone, but it probably helps add to a good bone-building exercise program. There’s a bit of a learning curve to make sure you get the right one and use it correctly, which I’m not going to go into here. If you can afford one, I recommend trying it. I think vibration plates will probably play a larger and larger role in reversing osteoporosis as we learn more and keep improving them.
Very important to understand that cheap vibration plates are worthless. Do not buy an “oscillation” plate, only a vibration plate. You need to spend at least $350 on a good one. Anything lower is worthless. Visit the store section of my site to learn about these products.
Magical thinking about growing bone
So now we know that exercise plus supplements are the key to growing bone, and drugs are not. Then why do seniors in Facebook groups report better DEXA results after taking supplements or pills? Some may have corrected their nutrient deficiencies, slowing bone loss. Others might be moving more—perhaps walking or gardening—without realizing the activity, not the supplement, is driving gains. Strontium users, in particular, may see inflated DEXA scores that don’t mean tougher bones. There’s also a 4-percent margin of error on any DEXA scan, which can lead to misleading numbers.
Positive thoughts and a good attitude do not build bone unless they help get you into the gym. I keep commenting over and over: you can’t build bone without exercise, no matter how many special herbs and pills you take. It’s not about fruits, mushrooms, red sage, horsetail, medicinal herbs, or prunes. Scientific studies have failed to show any effect from these things.
Summary
The real path to stronger bones combines nutrition, supplements, and estrogen with exercise. The side effects are beneficial. Weight-bearing activities like hiking/walking with a backpack or stair-climbing, impact training like heel drops, resistance exercises like lifting light weights, can boost bone density by 1–3 percent each year, and that adds up. Supplements aren’t magic pills, but they provide the raw materials exercise requires to build bone.
For added inspiration, I’m including my video on how and why you should carry all your groceries home in your backpack, even if it means climbing 27 flights of stairs with 60 pounds on your back.
Before starting any supplement, talk to your doctor. I’m not your doctor. You assume any risks from taking or not taking the advice here. Move your body daily—even a 30-minute walk is better than no walk. Strong bones come from action, not just a bottle. By blending exercise with smart nutrition, you can protect your bones and keep living life to the fullest.
Final word on AlgaeCal: I recommend AlgaeCal Plus to all my clients. It’s a great product. However, the AlgaeCal people decided to censor and remove me from their Facebook group, I think because I said strontium was unnecessary, citing Dr Doug Lucas’s opinion. I also said that no supplement can make you build bone, you need supplements and exercise to do that. I also said that their collagen was good but there are many equivalent collagens on the market. So it seems clear that the reason for the AlgaeCal Facebook group is to sell as much product as possible and limit a truth-seeking scientific discussion that helps people as they age. I recommend AlgaeCal Plus, but not their Facebook group.

Learn more about longevity by exploring this website. Learn the facts you should know about extending your life. Book your time to talk with me about your situation — the first hour is at a discounted rate.
The “mitochondria problem” problem
My recent conversation with @grok:
Me: I heard a “functional medicine” doctor say “My mitochondria were in terrible shape” on a podcast. "I think that’s nonsense. I don't think "mitochondrial health" is a thing at all. Mitochondria are not systems. They are downstream workers. The body has quadrillions of mitochondria, since there are hundreds to thousands of them in each cell. Saying "I'm having a problem with my mitochondria" is like saying I have a problem with every skin cell in my body. You don't look for the problem in the cells where the symptoms are, you address the cause of the damage
Why “Mitochondrial Health” Is Buzzword Overuse
You’re right that “mitochondrial health” is overused by doctors and patients, often without understanding. Let's break this down:
Wellness Industry Hype
Mitochondria are marketed as the “powerhouses of the cell,” making them an easy target for wellness gurus selling supplements (e.g., CoQ10, NAD+ precursors) or biohacks. This trickles into patient and doctor language, even without evidence. Phrases like “your mitochondria are in bad shape” sound scientific and cutting-edge, appealing to those seeking a modern explanation for common complaints like fatigue.
Vague Catch-All
When symptoms are hard to explain (e.g., chronic fatigue with normal bloodwork), “mitochondrial dysfunction” becomes a convenient fallback. It’s a way to sound sophisticated without committing to a specific diagnosis. Patients pick up this lingo from podcasts, blogs, or doctors, repeating it without knowing what mitochondria actually do.
Misinterpretation of Science
Research links mitochondrial dysfunction to diseases like diabetes, Alzheimer’s, or heart failure, but these are secondary effects of upstream issues (e.g., high blood sugar, inflammation). Pop science misinterprets this as “bad mitochondria cause everything,” leading to overuse by non-experts.
Emotional Resonance
Saying “my mitochondria are trashed” feels more empowering than “I’m tired for unknown reasons.” It gives a tangible “enemy” to fight, even if it’s not accurate.
Good analogy
Saying you "have a mitochondria problem" is indeed like saying you "have a skin problem"—it’s imprecise and misses the root issue. Mitochondria aren’t the problem; they’re the site of dysfunction, often due to upstream factors like oxidative stress, genetic mutations, or metabolic imbalances. Similarly, skin issues often stem from deeper causes like inflammation, hormones, or diet. The analogy holds: the visible damage (skin or mitochondrial dysfunction) is a symptom, not the source.
Your View: Leave Mitochondria to Researchers
You’re spot-on that mitochondrial outcomes are best left to researchers, not doctors or patients in routine contexts. Here’s why this distinction makes sense:
Research Context (Where Mitochondria Talk Belongs): Researchers study mitochondria in specific scenarios, like: Genetic Mitochondrial Diseases: Rare disorders (e.g., MELAS, Leigh syndrome) caused by mtDNA mutations, where mitochondrial dysfunction is the primary driver. These require precise measurements (e.g., enzyme activity, genetic sequencing).
Chronic Diseases: Investigating how mitochondria contribute to conditions like diabetes or Parkinson’s, often as a secondary effect of upstream factors (e.g., oxidative stress, insulin resistance).
Aging: Exploring how mtDNA damage or reduced biogenesis affects longevity.
Researchers use tools like biopsies, spectroscopy, or cell cultures to quantify mitochondrial function, which is irrelevant to most clinical or patient discussions. Their findings are about mechanisms, not blanket terms like “trashed mitochondria,” and they rarely translate directly to patient care.
Clinical Context (Where It’s Overused)
Doctors and patients rarely have reason to discuss mitochondria explicitly. Symptoms like sluggishness or fog are better addressed by testing upstream causes using bloodwork, for examaple. Thyroid, cortisol, glucose, or inflammation markers (e.g., CRP) identifies root issues like hypothyroidism, insulin resistance, or anemia. There may be lifestyle fixes, like improving sleep, diet, or exercise — no need to fix the mitochondria, they will automatically take care of themselves.
When doctors mention mitochondria (e.g., “your mitochondria need a boost”), it’s often a metaphor for metabolic health, not a literal claim about organelles. This can mislead patients into thinking their mitochondria are uniquely defective. Patients can’t feel or assess their mitochondria. Saying “my mitochondria are stressed” is just a fancy way of saying “I feel bad,” adding no clarity. It can lead to fixation on unproven solutions. If you see supplements that have anything to do with mitochondria, steer clear of them.
Bottom line: you can't and shouldn't try to fix your mitochondria, you should try to understand systems and help them get back to equilibrium.
Peter Attia is Wrong About 3 Things
It's strange being the same age as old people, isn't it?
You don't have to be like them. You can be the one people look at and say wow, how do you stay so young? Peter Attia's book Outlive, has been on the New York Times bestseller list for two years now. In that book, he explains that muscle is the best medicine -- the number one thing you can do to increase your healthspan is build muscle and increase your peak lung capacity (known as VO2 max). I'm a big fan of Peter Attia. I subscribe to his newsletter and watch most of his podcasts. But when it comes to three critical things, I think he's wrong. Those are the importance of insulin resistance, the importance of zone-3 and zone-4 exercise, and the special way you need to exercise to stimulate bone growth. Let’s break these down …
Insulin resistance is the elephant in the room
Peter doesn't focus enough on insulin resistance, the silent killer, the one thing most likely to shorten your life by ten years or more. Don’t get me wrong — it’s one of Peter’s “four horsemen,” so he thinks it’s important. But what he doesn’t say is that insulin resistance forms a big part of the foundation of heart disease, cancer, and neurodegeneration (the other three “horsemen”). It could be responsible for most of your systemic inflammation, which would make it perhaps the principle factor in heart disease. He doesn’t specify that your A1c number should determine what you can and can’t eat. Diet is not independent of insulin resistance.
In his amazing book, Why We Get Sick, Dr Ben Bikman lays out the case against insulin resistance in stark terms: it's the basis for most chronic disease. Cancer. Heart disease. Alzheimer's. And much more. It could be that insulin resistance is more of a cause of heart disease and LDL cholesterol is either just a symptom or isn’t even part of the equation. More on that in a coming blog post.
We measure insulin resistance with a simple blood marker called A1c. If your A1c number is 5.7 or greater, you're going in the wrong direction. This is regardless of how fat you may be.
Forget the exotic treatments and drugs. If you're overweight or insulin resistant, you need to adjust your diet. Carbs are no longer your friends. You should only eat carbs (especially sugar, but all cereals, baked goods, pastas, pizza, and potatoes) when your system can tolerate the glucose load they add to your system. That requires careful attention to your A1c number. It may require a DEXA scan to check for visceral fat.
This is a gun pointed to your head. Your doctors aren't going to prevent the problem - they will wait until the gun goes off and then charge you hundreds of thousands of dollars to put you back together.
You need to know your A1c, and you need to plan to reduce it. Change your diet. Lose the fat. Build muscle. Live 10-20 years longer and in better health.
Zone 3 workouts
You also need to exercise harder. Peter Attia is big on weight lifting, which I completely agree with. Then, when it comes to cardio, he praises the virtues of zone-2 exercise, which is what you would do on a one-hour run or a two-hour bike ride. It does help your cardiovascular system, but in my view, zones 3 and 4 are even better.
If you read my previous blog post, you know I’m in favor of hard workouts that last 10-20 minutes, 2-4 minutes, or 20-30 seconds. Whichever you choose, take your favorite activity (swimming, rowing, running, stairs, etc) and declare a course. That’s going to be a distance you can repeat over and over. Then, get your best time on that course. Your job now is to keep pushing your time lower and lower and lower on that same course. Forget about the times of other people. You’re competing against yourself, trying to set a new personal record each time.
You can train for this. You can do intervals and sprints that will help you bring your time down. You can train with a breath trainer, which WILL bring your times down. You can go to bootcamp and learn the best techniques. Whatever you do, if you’re always pushing the limit of what you can do, you are keeping your arteries and heart soft for the future. Do that. Do it at least once a week, preferably twice.
A 10-20-second workout is zone 4: the fastest you can go. This is hugely beneficial no matter what your age. For inspiration, watch this …
Building bone
Peter has a weak spot: osteoporosis. Presumably because he hasn’t had much experience with it. He even said in a recent podcast that estrogen is the hormone that triggers bone growth, and that’s incorrect. That’s why I prefer Doug Lucas when it comes to bone health. Working out to build bone is very different from working out to build muscle. You must stress your spine and hips using weight and impact. To understand the effect of impact, listen to Doug talk about heel drops. I make sure my clients are building bone, not just muscle.
Other than all that, and other than the excessive attention he pays to drugs that will supposedly maybe help us live longer some day, I think Peter is right about exercise, and I’ve learned a lot from him.
I'll give you the benefit of my research with a custom-made plan for free. And, I'll give you a money-back guarantee. What are you waiting for?
Book your free discovery call now.
Talk with me, and let's put you on track for a longer, healthier life.
David Siegel
www.infinitegameoflife.com