What's wrong with the senior-care market and what I plan to do about it:

I’ve been giving talks at senior communities around the DC area, meeting the administrators, residents, touring the facilities, giving talks. It’s disheartening. I can help most people over 50 live 5-20 years longer. But there isn’t much demand — yet.
In this essay, I’m going to make a number of observations, give some background, and suggest how we can help people over 50 live much higher-quality lives. At the end, I’ll explain how you can help turn this into a serious business, especially if you’re a marketer or investor.
Let’s start with what I think is going on …
People are aging very poorly. We are behaving ourselves to death. Life expectancy, already low in the US, is heading down. It's not about economics, it's that the healthcare system is designed to suck money out of people at the wrong time — after they have a catastrophic event — rather than prevent it. And it’s that Americans are consuming more delicious food and becoming less active. There are other factors involved, but the numbers are not pretty …

The US has by far the most expensive healthcare system in the world, spending $12,000 per person each year, and getting the worst results of the top 25 developed countries. People in China live longer than Americans for 10 percent of the price, not because their medical system is better but because Chinese people are used to hard work and stay active. Americans are spending more money to move less, and that’s what’s causing the problem.
Retirement communities are giving retirees what they want, not what they need. These communities are all very similar. They are very comfortable. The food is plentiful and delicious. They have “activities,” gentle yoga, a bit of movement. People lift 3-pound dumbbells or do some gentle water activities, pretending they are exercising. This is physical abuse — our bodies aren’t designed for it. Yet, if a retirement community advertised that they would get you down to a normal weight, work with you to build muscle, no sugar, no alcohol, get stronger, and no treats except on birthdays — no one would join that community. The company would either go out of business or they would have to convert back to what we have today, because people won’t buy future health, they want to buy comfort.
People over 60 are eating more and moving less. They aren't challenged. They are living peaceful, calm lives and eating cake. Citydwellers are in far more danger than if they would just go to a farm or a ranch and get a job as a helper.
Longevity nerds are very few and very visible. There is a very small number of longevity nerds, but they make a lot of noise. They are YouTube influencers, investors, conference-goers, entrepreneurs, and Facebook group starters. Even though Peter Attia’s book Outlive has been on the NYT bestseller list for two years now, the actual number of people interested in doing something to improve their health is remarkably small. There’s a real market here, but it’s just getting started.
Because of one very expensive and very bad study that made headlines in 2002, women don't know anything about hormone replacement. After 50, their estrogen and progesterone plummet, and many don't even talk with a doctor about trying to replace them. Most doctors are unqualified. So 95 percent of women aren't getting the many life-saving benefits of hormone therapy — a public health failure.
Seventy five percent of American adults are overweight or obese. They think it's normal to keep buying clothes in bigger sizes. When it comes time to start injecting insulin, they order their supplies and start doing it five times every day. I ask them: “Would you like to stop injecting?” They say, “Sure, of course.” Then I tell them it’s going to take hard work for 6-12 months and lose weight, and they say “Nah, I’ll pass.”
People don't know anything about insulin resistance. Insulin resistance increases your chances of heart disease, cancer, Alzheimer’s, and gaining weight. Most people are insulin resistant, unhealthy, and are taking idiotic dietary advice that makes them sicker. They think they got unlucky and got cancer, but they brought it on with a poor diet. Everyone over 60 should know his/her A1c number from a test in the last six months. When I ask how many know their A1c number, usually only one person raises a hand — the person who’s on medication for insulin resistance. Even the diabetics don’t know their A1c number, nor do the staff don’t know their own A1c numbers. This number should drive most of your health decisions.
No keto awareness. If more than 50 percent of residents are seriously overweight, then the facility needs a keto option and most of the residents should be on it. In my lectures, I ask people if they know what keto is and they all shake their heads, including the staff (many of whom should also be on a keto diet). They are getting the wrong advice.
If residents cared to get better, they could wear a button on their clothing at all times showing their A1c number. Not a badge of shame, but a badge of courage. As people get tested and their numbers change, they trade the button in for a new one, so people can see they are making progress. It also tells staff to remind them if they order carbs or sodas or desserts that they won’t be helping themselves get the next lower numbered button. Obviously, if people want to be diabetic, they won’t wear the button, but if you’re wearing the button, you’re asking the staff to help you make good choices.
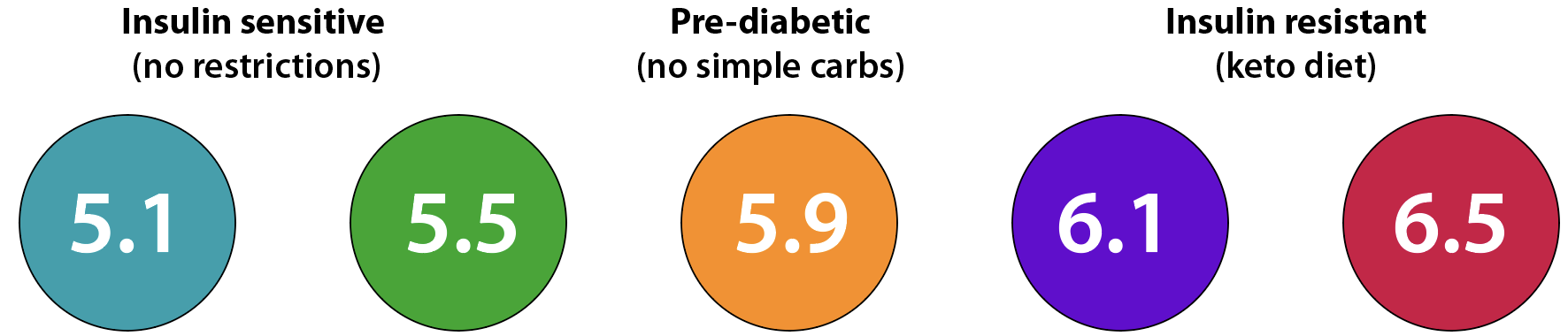
Know your A1c number and show others you are working to lower it.
Half of all heart attacks and strokes occur before age 65, yet people in their 40s and 50s have no idea what's about to happen. They aren't taking care of themselves -- they are too busy. They think when they get a heart attack they were just unlucky, and that’s when they spend hundreds of thousands of dollars to try to go back the way they were before.
No bone-building programs. This is so easy to do, yet no one does it. To learn more, read my big essay on bone building and watch the accompanying video. I have many ideas how people can do this easily and cheaply.
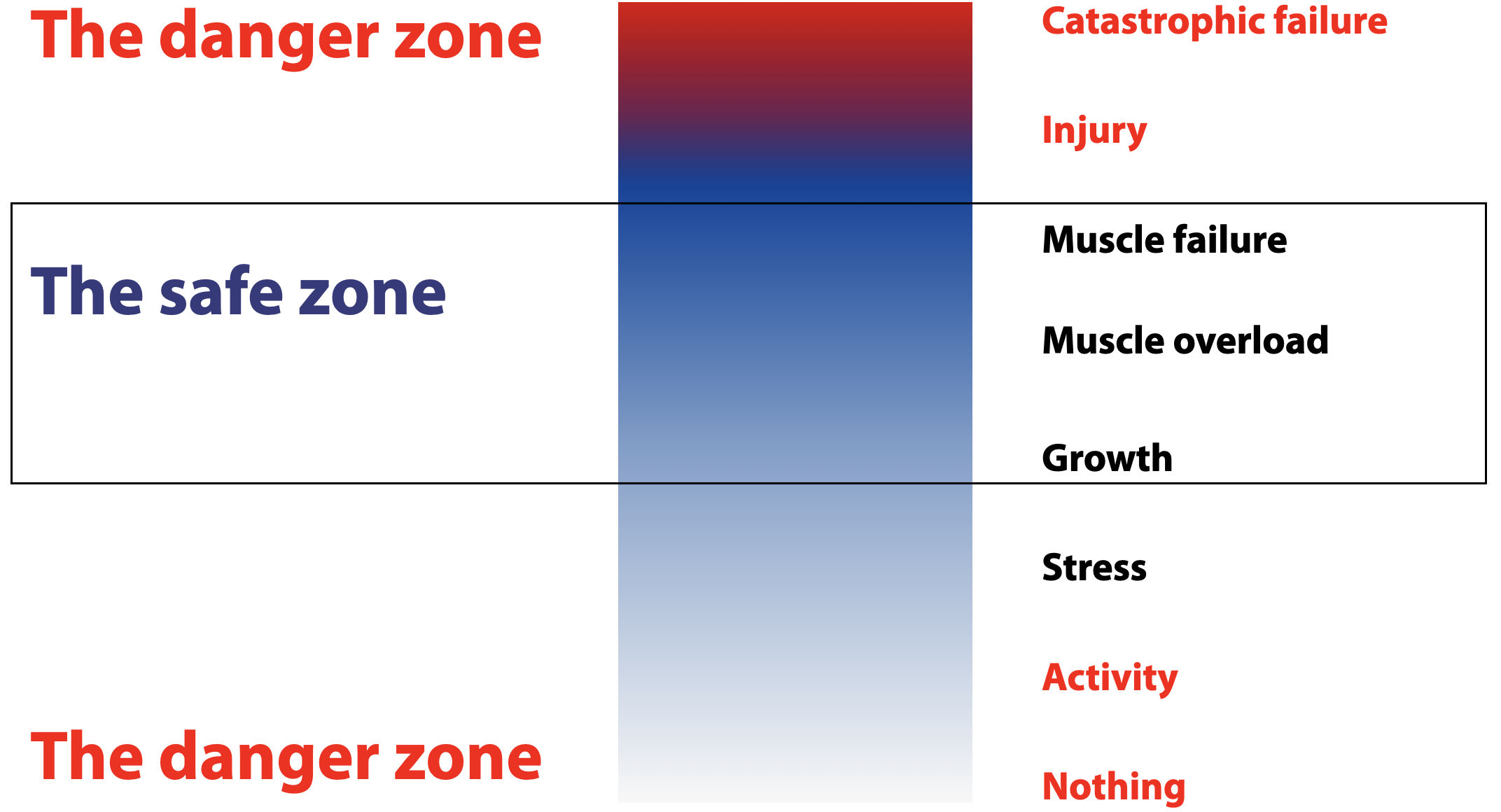
Everything is medicalized. You can get off the blood-pressure medication and reduce your A1c and your risk of heart disease by exercising. More exercise is better. Harder exercise is better. Pretending to exercise is not better. I show this slide to help people understand where the real risks are:
More than half of all doctors are out of date and routinely prescribe what big drug companies want them to prescribe. Why? Because patients would rather have medicine to lower blood pressure than do any exercise. They want drugs for everything, so that’s what doctors give them. Many common drugs and treatments don’t work, but some do. Only 15 percent of doctors are statistically literate — the rest can't pass a simple biostatistics quiz.
Outdated Practices & Ineffective Care. Studies show many medical practices are simply out of date and provide little to no benefit to patients, though many make money for doctors. One in eight studies leading to common medical recommendations has already been shown to be ineffective, yet doctors keep prescribing them. Only about 50 percent of doctors consistently follow current evidence. Fewer than 40 percent of doctors recommend exercise, because fewer than 40 percent of doctors exercise regularly themselves. Many surgeries (e.g., spinal fusions, stents) show no benefit over placebo, yet remain common.
Too many drugs are overprescribed. Here’s a short top-ten list:
Proton Pump Inhibitors (e.g., Omeprazole): For GERD; long-term use (>8 weeks) often lacks benefit, increases risks of kidney disease, fractures.
Antidepressants (e.g., Sertraline): For mild/subsyndromal depression; 50% of patients see no benefit, with risks of emotional blunting, sexual dysfunction.
Levothyroxine For subclinical hypothyroidism; no clear benefit in mild cases (TSH <10 mIU/L), yet widely prescribed, risking overtreatment.
Benzodiazepines (e.g., Lorazepam): For anxiety/insomnia; long-term use ineffective, increases fall risk (elderly) and dependence. ~30% of older adults overprescribed.
Antipsychotics (e.g., Risperidone): Off-label for dementia behavior; no consistent benefit, increases mortality risk in elderly (1–2% higher).
Bisphosphonates (Fosamax, Boniva, Actonel): For osteoporosis; long-term use (>5 years) may cause jaw osteonecrosis (1/10,000–100,000 risk), atypical femur fractures. Does not grow bone but prevents bone loss in an unhealthy way.
Antihypertensives (e.g., Lisinopril, Hydrochlorothiazide): no clear benefit in low-risk patients, risks hypotension, falls in elderly, and exercise replaces most.
Metformin For prediabetes or off-label (e.g., PCOS); minimal benefit vs. lifestyle changes (26% reduced diabetes incidence), risks GI issues, lactic acidosis (rare). Changing diet and exercise do the job better.
Statins (e.g., Atorvastatin): For low-risk patients, 20–30% see no cardiovascular event prevention (NNT 217 for heart attacks), with risks of muscle pain, diabetes.
NSAIDs (e.g., Ibuprofen, aspirin): For chronic pain; long-term use risks GI bleeding, kidney damage with minimal benefit over non-drug therapies.
Anticholinergics (e.g., Oxybutynin): For overactive bladder; marginal benefit in elderly, increases cognitive decline risk.
Gabapentinoids (e.g., Gabapentin): For chronic pain; limited efficacy for non-neuropathic pain, risks sedation, dizziness.
Half of all medical tests are unnecessary. We spend $200 billion a year on routine checkups that do nothing but make money for doctors. On the other hand, the new “functional medicine” people love to order tons of tests, saying “We check over 150 biomarkers.” Testing that many things is going to show some number or other is low or high, and that’s when the drugs and treatments start. It’s now fashionable to offer full-body scans that just make people worried about some little dark spot on a scan that later turns out to be nothing important. In many cases, the cure is worse than the disease.
People are going the wrong direction. They are gaining weight and losing muscle. I ask “How many people here can get up out of a chair without using your hands?” Usually about half the people can do that. Then I ask “How many of you would like to be able to do that in five years?” They hadn’t thought about that. Half of them won’t be able to. The less strength you have, the more limited your options.

About 60 percent of Americans in their 70s can get up without hands, but only about 35 percent can do so after age 80.
Lack of equipment. More than half of all senior-care facilities don’t really have any equipment at all. They have a few bands and dumbbells in a box. The staff aren’t trained properly. There is no program, there are just some activities that look like people are moving - gentle yoga, some pool exercises, some stretching. If these programs worked, people would not be gaining weight, but they are gaining weight. They are not getting stronger. Facilities with a gym have a fairly standard gym that isn’t geared to promoting strength and conditioning for older people. Facility owners have no idea what to install, so they put in some machines that look good on a sales tour or that are designed for rehab. I know one building where all the equipment has to be black, so the gym looks good in photos. A perfect example is that every gym should have parallel railings and wedges and benches so people can practice squatting and getting back up — this is almost nonexistent.
No ping pong. This is a disaster. Ping pong is one of the things older people can do to maintain and even improve hand-eye coordination. Yet management does not prioritize this or thinks it may be too dangerous. Ping pong helps keep people safe, because it develops reflexes that help prevent falls. They should have competitions, leader boards, and tournaments around the city. There should be state, regional, and national championships. People should be excited to improve their ping-pong skills and want to improve their rankings. All the other stuff is too slow.
Lack of motivation. People don’t use the gyms or move much, and instructors aren’t there to push them. People don’t have projects or goals, they have activities. They look forward to birthday parties rather than competitions or fitness goals. Sir Rod Stewart is now 81. He runs 100 meters in 19 seconds, and he has a goal of 17 seconds. How many people are that motivated at his age?

At age 81, Rod Stewart can run 100m in 19 seconds.
Noise in the longevity channel. Now there are billions of dollars pouring into longevity, but most of the money is going toward 1) exotic drugs that have never been shown to extend life in humans, and 2) exotic expensive treatments for rich people that are highly medicalized and do not provide longevity. Examples:
Canyon Ranch offers a 4-day, $20,000 “longevity” program that gives wealthy people a lot of attention, too many medical tests, and no lifestyle changes.
Equinox is launching a $40,000 per year longevity program. They are partnering with Function Health to measure too many things and pay too much attention to the medical side of longevity. It’s probably the first viable program I’ve seen that will help improve longevity, because they will focus on fitness. But will they have the programs I advocate, especially hormones and bone-building? Probably not. It seems aimed at people in their 40s and 50s. I hope it goes well — we need more awareness of fitness and less medicalization for longevity.
Blue Zones Center Miami is an ultra-exclusive, high-end medical treatment center designed to suck money out of rich people. No longevity will come of this. It may help catch a few cancers early, at the expense of many false positives and unnecessary treatments. I hope it fails miserably and bankrupts its investors.
How to fix this?
In my view, this is a crisis, because it is so preventable and probably costs less than what we’re doing now. Senior-living facilities are giving the market what it wants. The root problem is that there’s very little demand for prevention. But that can change. There are three things we should do immediately:
Competitive ping pong for every senior community. It doesn’t matter what the income level is. Ping pong is not difficult or expensive to set up, and a program is not that hard to put together. Residents need training, leaderboards, competitions, championships, and recognition. There should be dominant-hand games as well as non-dominant-hand competition. There is no excuse not to do this immediately.

Start longevity programs in each retirement community. These will be aimed at about 20 percent of residents who learn that they have a choice. They want a program, want to lose weight, want to get stronger, and want to increase healthspan. They need support. They would pay extra for a daily program that gives them individual consultation, individual fitness coaching, and a group class. This would take place every morning from 9am to noon or in the afternoons from 2-5pm (so the coach can go to another facility on the same day). The rest of the time, they are on their own, but they have assignments to do, goals to achieve, progress to track, and they wear their A1c badge, so everyone in the community agrees to support them in improving their health and reducing dependence on doctors. I propose to provide that program as an outsourced contractor service.
Start a few longevity-themed pilot projects. A few dozen senior communities around the country should commit to starting a program as I just described, with the goal of phasing that program in 100 percent, so that community becomes the longevity-focused community for its metro area. This will involve a completely different kind of gym, menu, even stairways. I’d like to see half a dozen pilot programs get going on this in 2026.
In the long run
Over the next ten years, senior living will start to shift significantly, not just because we know more what works but because future seniors are going to demand it. I have written a separate essay on the senior-living center of the future.
Cities like Miami Beach are now creating “Blue Zones” that they hope will attract people for the new healthy lifestyle they want to create. These cities have become victims of Dan Buettner, who coined the term blue zone and is now using it as a marketing tool to make money. He charges a huge amount of money to make these gorgeous reports that are excellent sales tools. There’s a lot of value here, because so many cities are in need of attention. As I have written to the people of Miami Beach: “Many good things will come of this, but longevity is not one of them.”
I would also like to talk with apartment-building developers, because they could offer longevity gyms and longevity programs that will attract buyers and renters to a more healthy and fitness-oriented lifestyle. A luxury condo building with a longevity program and specially designed gym will stand out among all the buildings with Euro-kitchens and floor-to-ceiling windows. I have a full business plan for this and can build the longevity gym to suit and run the program for any developer.

Want to work with me?
I believe I can create the disruptive category-leader company in longevity, because I’m actually focusing on health and longevity rather than medical tourism and pampering. But it takes more than I’m doing now. It takes a team. Here’s what I’m looking for:
Marketing. People pay for what they want, not what they need. Most people in their 60s would rather take a vacation to Vegas than invest in their own health. I think more women are concerned about their hair than about hormone replacement therapy (which would help improve their hair a lot). I’m surprised how little people care about their own health and how most people’s plan is to put it off until something catastrophic happens, then let the doctors deal with it. About 3 percent of the population is very fitness aware and already working on longevity, and 75 percent are passing up opportunities to become more healthy every day. That leaves roughly ten percent of people who can afford and would be open to extending their healthspan. These are my customers. I can get them, I just need to try more things and find what works. I want to do events, funnels, direct outreach, Instagram, Twitter, partnerships, institutional contracting, and more. Want to help? Get in touch.
Connections to investors. I hope to raise $250,000 from accredited investors to build all the funnels, online events, and client-acquisition systems. As we say in business, sales solves most problems. With more money I’ll focus on more sales, which will let me continue to hire, build, and scale. If you know any accredited investor who would like to talk with me, please introduce us.
Consultants in various markets. I’m looking for people in San Diego, Los Angeles, San Fernando Valley, Santa Barbara, Austin, and possibly Phoenix. These would be people I train to work with clients in senior communities in those metro areas. This is not online, this is going to communities to work with people 60 and up.
Contacts of corporate wellness directors at Vi Living, Atria, Leisure Care, Sunrise, Five Star, Ritz Carlton residences, W residences, Four Seasons residences, Miraval, and others.
Contacts at luxury building developers (condos, rentals) like Bosa Development and others.
If this is your first time here, go to the Facts page or explore the blog.